Anemia
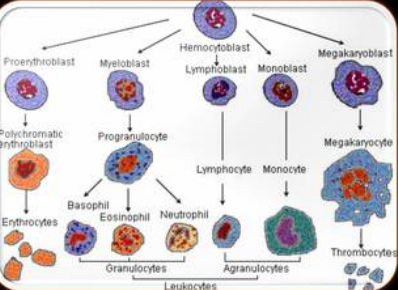
Red blood cells
Normal Values:
Hemoglobin range Men : 13 - 18 Women : 12 - 17
Hematocrit range Men : 40 - 50 Women : 37 - 47
Tired Blood’ Warning: Ignore It at Your Peril
By Jane E. Brody : NY Times Article : July 19, 2008
Thanks to advertisements for the once-popular tonic Geritol, most people of a certain age know about “tired blood,” a disorder more accurately called anemia, involving a shortage of healthy red blood cells to carry oxygen to body tissues and cleanse them of carbon dioxide.
It is not really the blood of people with anemia that is “tired.” Rather, it is anemic people themselves who commonly experience chronic fatigue. Other symptoms may include weakness, shortness of breath, impaired athletic performance, rapid heartbeat, irritability, apathy, dizziness, pale skin, headache and numb or cold hands and feet. But in many people the symptoms are too mild to be recognized, and the anemia goes undetected for years.
Anemia is the most common blood disorder in the United States. Statistics indicate that 3.4 million Americans are anemic, but experts say that this is a gross underestimate and that anemia has been viewed for far too long as an “innocent bystander,” considered almost normal in certain groups, like menstruating women and the elderly.
But a growing body of research indicates that anemia can seriously compromise the quality of a person’s life, make sick people sicker and even speed deaths, said Dr. Allen Nissenson, a nephrologist and professor of medicine at the University of California, Los Angeles.
It is time to take anemia much more seriously, he added, making sure people have routine blood tests and are treated to restore healthy supplies of red blood cells. The testing is done either by a finger prick or by drawing blood from a vein. The finger test usually measures the hematocrit level, or percentage of red blood cells in plasma. A normal count is 36 percent to 46 percent for women and 46 percent to 56 percent for men.
A more accurate assessment measures the oxygen-carrying hemoglobin in blood, expressed as grams of hemoglobin per deciliter of blood. A normal hemoglobin for women is 12 to 13 grams, and for men, 13 to 14. Hemoglobin has traditionally been measured in blood from a vein, but a finger-prick test is now available.
Inadequate nutrition is the most common cause of anemia, Dr. Nissenson said. Production of hemoglobin, the oxygen-carrying protein on red blood cells, depends upon the mineral nutrient iron, most prominent in meat and poultry (especially organs like liver and kidneys) and egg yolks.
To a lesser degree, it is found in green leafy vegetables, dried fruits, dried beans and peas and enriched and whole grain cereals and bread. Foods rich in vitamin C help the body to absorb iron.
Also important to the production of healthy red cells are B vitamins, folic acid, B12 and B6. B12 occurs only in animal foods, especially meat, fish, eggs and milk. Dark green leafy vegetables are the best source of folic acid; whole grains are the best source of B6.
These nutrients are often in short supply among women who lose iron in menstrual blood, pregnant women, strict vegetarians, overly zealous dieters and poor people. Increasingly, the problem is found among elderly people on restricted diets.
Anemia afflicts virtually everyone with kidney disease because shrinking kidneys are not able to make enough of the hormone erythropoietin, which controls the production of red blood cells in the bone marrow. In addition, many chronic diseases involving inflammation can result in anemia, including congestive heart failure, inflammatory bowel disease, rheumatoid arthritis, AIDS, liver disease and cancer.
There are also hereditary anemias like sickle cell and thalassemia, and hemolytic anemias that involve the destruction of red blood cells faster than they can be replaced. Immune disorders and medicines can also bring it on.
Anemia can also result from chronic blood loss — from an ulcer, polyp or hemorrhoid — that may not be apparent without a stool test. Occasionally, a previously undetected cancer in the digestive tract can be the cause, so if no other responsible factor is identified, a colonoscopy should be done.
Doctors have long been aware of the risk of anemia in infants and in teenage girls and women of childbearing age, but anemia is far more prevalent in people over 65, studies say. One concluded that the incidence of anemia among the elderly was four to six times as great as had been suspected, affecting as many as a quarter of those over 75.
Even among patients with nearly identical medical disorders, those who are anemic tend to die faster. In one study of Medicare patients with congestive heart failure, for example, for every 1 percent decrease in the hematocrit (or percentage of red blood cells in plasma), the mortality rate rose by 1.6 percent.
In a study of nearly 79,000 elderly patients hospitalized with heart attacks, blood transfusions greatly lowered the death rate among those with hematocrits of less than 33 percent upon admission to the hospital.
Likewise with dialysis patients. In a study of 20,000 such patients with chronic kidney failure, those who were more severely anemic had a death rate twice that of patients less anemic. But when anemia in dialysis patients was treated effectively, the death rate after one year was no different from the rate in those who were not initially anemic.
Cancer patients also seem to do better when they are not anemic. Chemotherapy and radiation often cause anemia, which is associated with a reduced ability to control the disease and a lower survival rate.
Perhaps the most common consequence of anemia is an impaired quality of life, especially among older, ostensibly healthy people. In a study published in The American Journal of Medicine, Dr. Brenda W. J. H. Penninx and co-authors followed a group of 1,146 men and women 71 and older for more than four years.
The participants performed three tests at the start and end of the study: standing balance, a timed eight-foot walk and rising from a chair. Those with hemoglobin levels just slightly below normal were one and a half times as likely to experience physical declines as those with normal hemoglobin. Those with greater degrees of anemia experienced greater declines.
“Although no study yet shows that treating anemia in older people reduces the incidence of physical decline, our study certainly suggests that this may be the case,” Dr. Penninx said.
Anemia treatment is mainly determined by the cause: correcting underlying disorders, changing diets, adding nutritional supplements and for many, costly genetically engineered drugs like Procrit, Epogen and Aranesp.
Updated from an article that appeared in The Times on Sept. 23, 2003.
New Anemia Treatments Bring New Problems
By Eric Sabo : NY Times Article
Some forms of anemia, like those from nutritional deficiencies or bleeding, can be corrected by fixing the underlying problem. But anemia from cancer and chronic ailments like kidney disease are far more complex and can require years of specific treatment. Cancer patients, for example, face severe nausea and other side effects from chemotherapy, but they rate the tiredness from anemia as the most bothersome part of living with the disease.
Studies show that fatigued patients with anemia feel more energized after receiving transfusions of donated red blood cells, a procedure that has been around since the 16th century. But the process is laborious, and transfusions carry serious risks like emerging infectious diseases, mismatched blood types or fluid buildup in the lungs.
In recent years, doctors have found that newer anemia drugs like Procrit and Aranesp could produce roughly the same effects as transfusions, but with greater ease and seemingly less risk. The medications, which are also injected but in less time, made a lasting impact on many fatigued patients, who say they regained at least some of their old vigor when little else worked. Prescriptions for the drugs soared.
Yet the top-selling medications are undergoing a serious reappraisal after being linked to higher rates of heart attacks, stroke and early death. Early in 2008, the Food and Drug Administration’s scientific advisory board issued strict new warnings on the drugs, saying that higher than normal doses can lead to heart problems and also promote tumor growth in certain cancers. It was the second such warning that the F.D.A. had issued on the treatments in nearly a year.
“I think people need to be extremely cautious with the use of these drugs,” said Dr. Allen Nissenson of the University of California, Los Angeles. “At a minimum, patients should be satisfied with modest improvements from low doses as a way to minimize the risks.”
Dr. Douglas Rizzo, who directs the Center for International Blood and Marrow Transplant Research at the Medical College of Wisconsin, said it was still unclear whether high doses were at the root of the problem. The drugs stimulate production of erythropoietin, a hormone that helps blood cells ferry oxygen. But the natural energy booster also plays other roles in the body, including healing wounds, and making it a drug target could produce a range of unknown effects, he said.
“There’s a lot of uncertainty,” Dr. Rizzo said. “I think patients will have a difficult choice to make.”
And it’s not always a choice. A study published in The New England Journal of Medicine found that anemia drugs did not completely replace the use of transfusions in critically ill patients, so some people end up requiring both forms of treatment.
The only natural option, Dr. Nissenson said, is to move to higher ground. “It’s not a joke,” he said. Living at high altitude for a period of time stimulates the production of red blood cells to compensate for the lack of oxygen in mountainous areas.
“You don’t need to go to Mount Everest,” Dr. Nissenson said. “If you look at people in Denver, Colorado their average hemoglobin is significantly higher than people at sea level.”
The Challenges of Anemia: Defining It, and Living With It
By Eric Sabo : NY Times Article : July 19, 2008
Dr. Allen Nissenson is a professor of medicine and director of the dialysis program for the David Geffen School of Medicine at the University of California, Los Angeles. He has written two medical textbooks on kidney disease treatment and was president of the National Anemia Action Council, a patient advocacy group.
Q: Anemia can result from a wide range of diseases and conditions. What are the most prominent causes?
A: And then there’s cancer itself, or the side effects from treating cancer, that can cause anemia. Another prominent cause is deficiencies in erythropoietin, or Epo, a hormone that stimulates red blood cell production, which is almost entirely a problem in people with kidney disease.
Q: A lot of symptoms of anemia share the same characteristics as being overworked or just tired. How do you tell the difference between normal fatigue and anemia?
A: You really can’t. One of the dilemmas with anemia is that the symptoms are pretty ubiquitous: tiredness, weakness, some difficulty in thinking clearly. They’re all kind of vague.
So what we tell people is if you have these symptoms and they go on for a long time or seem to be interfering with your ability to function normally, then you should see your doctor. One of the things you need to get checked is your hemoglobin level — the protein that carries oxygen in red blood cells — to see if that’s part of the anemia.
Q: Is there a specific cutoff point of hemoglobin that indicates whether someone is anemic?
A: One of the challenges is defining what normal is, and there’s no uniform acceptance of normal hemoglobin levels. The one most doctors use is from the World Health Organization. A hemoglobin level below 13 for men and below 12 for women is considered anemic.
Q: Nutritional deficiencies are a common cause of anemia. Do these arise from a poor diet or underlying disease?
A: Bleeding is one of the most prominent causes of iron deficiency, because when you bleed you lose red blood cells that contain iron. But there still is a significant prevalence of nutritional iron deficiencies, which is much more common in pregnant women and children because of their diets.
Nutritional iron deficiency is the biggest cause of anemia worldwide, and it’s a problem is some segments of the United States. For folate or vitamin B12, it’s much less common to be deficient.
Q: How difficult is to live with anemia?
A: It’s very tough. One of the things we learned, however, is that the ability of the body to adapt is tremendous. Over time, even people with moderately severe anemia say, “You know, I really don’t feel that bad.”
Although people are fatigued or can’t do as much as they could before, they slowly adapt their lifestyle. Instead of walking to the grocery store once a week, they may go once a month and buy everything they need because they’re too tired to keep going back. There’s a lot of adaptation that takes place, but anemia can be very debilitating.
Q: Is anemia life-threatening?
A: The only life-threatening anemia is if you have massive hemorrhaging. But chronic anemia can be life-threatening indirectly in the sense that prolonged, severe anemia can cause the heart to enlarge and overwork, leading to heart failure. So through that mechanism, anemia can lead to serious morbidity or mortality.
Q: The Food and Drug Administration has issued warnings on three similar anemia drugs: Procrit, Aranasep and Epogen. How safe are these to use?
A: The studies that raised the red flags were either in cancer patients or in people with kidney disease, and they all showed something similar: if you attempt to correct the anemia completely back up to normal hemoglobin levels, that’s not a good idea. You start getting strokes or heart attacks, blood-clotting problems or increased mortality.
The recent studies that the F.D.A. flagged were just studies. Kidney specialists weren’t practicing this way — they were waiting for the studies. So we’re going to continue practicing the way we were, which is to give modest doses of the drugs, with modest improvements in hemoglobin.
Q: Are the drugs potentially dangerous for the elderly or other groups?
A: There are no studies to help us figure that out. There’s no question that since cancer patients and kidney patients are so different, but the same problem has arisen, I think people need to be extremely cautious with the use of these drugs.
One dilemma now is that if someone wanted to do a study on normalizing hemoglobin levels in the elderly with these drugs, I think an institutional review board that has to approve the ethics of studies like this would have a very difficult time because of the concerns of the risks.
Q: The F.D.A. says the drugs are safe to use in small doses that keep oxygen-carrying hemoglobin just below a level that is considered normal. Is this enough to help anemia patients feel better?
A: The quality of life benefit is seen with pretty modest increases of hemoglobin. It looks like you get the biggest bang for the buck early on. If you push the doses, then you start to see the toxicity.
Q: Are red blood cell transfusions a potentially safer option given the new concerns about the drugs?
A: As long as you’re aiming for a moderate increase in hemoglobin, the drugs are so much simpler and have few or any side effects unless you start pushing them hard. Whereas with transfusions, you still have the risk of infectious diseases and other issues.
Q: Are there lifestyle measures, like diet or exercise, that can treat anemia?
A: In the chronic conditions, there is probably very little that can be done. Obviously for nutritional anemia, improving nutrition will help. Probably the only thing you can do is to go to a higher altitude, because there’s less oxygen available.
As a result, the cells that make Epo detect that and then stimulate Epo to make more red blood cells. Even people with chronic illnesses have slightly higher hemoglobin when they go to altitude for a period of time.
What to Ask About Anemia
By Eric Sabo : NY Times Article : July 19, 2008
Confronting a new diagnosis can be frightening — and because research changes so often, confusing. Here are some questions you may not think to ask your doctor, along with notes on why they’re important.
How do I know if my fatigue is caused by anemia?
A physical exam will help determine the severity of your fatigue, along with other symptoms like weakness or difficulty concentrating. Doctors then test the level of hemoglobin in your blood, a substance that helps red blood cells carry oxygen to the body’s tissues, giving you strength. Persistent fatigue and lower than normal hemoglobin levels mean that you have anemia. Some doctors may also test your hematocrit level, which measures how much of your blood is made up of red blood cells. Low hematocrit is a further indication of anemia.
Can I get anemia from not eating properly?
Diets low in iron, vitamin B12 or folate can lead to anemia. But these nutrients are plentiful in most foods, and it does not take a significant amount of them to return nutrient levels to normal. Good sources of iron include red meats like liver, as well as poultry, fish, eggs, spinach and peas. The same types of animal products also contain B12, and most breakfast cereals are now specially fortified with the vitamin. Folate is a form of vitamin B found in breads, pasta and leafy vegetables.
Am I at risk for anemia if it runs in my family?
A small portion of anemias can be passed on to children at birth, namely thalassemias and sickle cell anemia. These are inherited genetic disorders that can cause the body to make fewer healthy red blood cells and less hemoglobin.
What diseases cause anemia?
Several chronic diseases can cause anemia, including rheumatoid arthritis and other inflammatory disorders that block the body’s ability to absorb iron. Virtually everyone with a long-term kidney disorder suffers from anemia because the kidneys are not able to make enough erythropoietin, which controls the production of red blood cells. Anemia is also prevalent in cancer patients, both from the disease and treatments like chemotherapy. People with heart disease or AIDS also often suffer from anemia.
How dangerous is anemia?
Anemia is not directly life-threatening unless it is linked to serious bleeding. But over time, anemia can cause the heart to overwork to compensate for the lack of energy. Patients with anemia tend to live shorter lives than those who suffer the same chronic diseases but without the fatigue.
Will anemia clear up over time?
Yes, as long as the underlying condition that caused the anemia is taken care of. Cancer patients who suffer from anemia, for example, may return to normal once their disease is in remission and treatment stops. Nutritional anemias are often easy to correct, with most people quickly returning to normal once they begin eating a proper diet.
Which anemia treatment should I use?
Iron supplements may be used if you are deficient in iron, either from a poor diet or chronic bleeding. The main treatment for many forms of anemia is using a drug to stimulate erythropoietin. The other major option is a red blood cell transfusion, which involves transferring donated oxygen-carrying blood cells to the anemic patient. Both treatments can improve symptoms of fatigue, but they are not a cure.
Are anemia drugs safe to use if I have cancer?
The Food and Drug Administration issued strict new precautions on anemia drugs after several studies found that higher-than-normal doses of the medications speeded tumor growth and shortened the lives of cancer patients. Those with breast cancer or cancers of the head and neck appear to have the highest risk and should consider forgoing the drugs altogether, a majority of experts convened by the F.D.A. recently advised.
In other tumor types, only patients receiving chemotherapy should take the drugs, because those who used anemia medications when they were not treating their cancer had higher rates of death. The F.D.A. recommends that cancer patients talk to their doctors about the risks and benefits of other options like red blood cell transfusions.
Are anemia drugs safe if I have kidney disease?
Many experts say that the benefits still outweigh the risks for people with kidney problems, as long as the drugs are used in moderate doses with modest aims. Studies have reported a higher number of deaths, nonfatal heart attacks, strokes and blood clots with high doses. The dangers appear to show up only after hemoglobin levels reach near-normal levels. Nearly everyone with kidney disease suffers anemia, and even modest improvements may restore some normalcy to people’s lives.
Are blood cell transfusions safe, and when should they be used?
Transfusions are routinely used to replace blood lost from serious injuries and during surgeries. They are also a common treatment for serious types of anemia, like sickle cell disease. But doctors consider transfusions a treatment of last resort for less severe anemia, because there is always a chance for spreading infectious disease and patients sometimes are matched with the wrong blood type. Better screening methods have significantly lowered these risks, but chronic anemia suffers may need several blood transfers, and the procedures are linked to greater problems the more they are used.
Can lifestyle measures treat anemia?
Nutritional anemias can be cleared up by getting more iron and vitamins. Researchers are studying whether exercise and special diets may increase energy in anemia patients, much like the benefits found in a range of other conditions. Living at higher altitude for a period of time is linked to naturally higher levels of hemoglobin and may help people feel less tired.
A: The biggest categories are nutritional anemias, which are mainly iron deficiency, but also deficiencies in folic acid or vitamin B12. Another major cause is bleeding, usually from the gastrointestinal tract. Chronic diseases that have an inflammatory component, like rheumatoid arthritis, can also cause anemia.
5 Things To Know Tips for Taking On Anemia
By Eric Sabo : NY Times Article : July 19, 2008
Dr. Lawrence Goodnough is the director of transfusion services at the Stanford University Medical Center and was president of the Society for the Advancement of Blood Management, a group that promotes better anemia control. He says that anemia is a serious medical condition, especially for people who suffer fatigue from chronic diseases. Here are the five things he believes everyone should know about managing the most common blood disorder.
1. Recognize the symptoms.
Headaches, dizziness, difficulty thinking and fatigue are the hallmarks of anemia. If these symptoms persist, see a doctor for a blood test. Having a low level of hemoglobin — the oxygen-carrying part of blood — can help determine if you suffer from anemia.
2. Take anemia seriously.
Everyone experiences fatigue from time to time, but anemia can sap your energy for long periods and keep you from doing the things you like. The symptoms may indicate an underlying bleeding problem that needs to be taken care of. Treatment for nutritional anemias can be as simple as getting more iron, vitamin B12 or folate, which are plentiful in most diets. More serious anemic conditions, like those caused by chronic diseases, may require special drugs or blood transfusions.
3. Get a blood test before surgery.
Doctors will test your hemoglobin levels a day or two before surgery because low levels could raise the risk of bleeding complications. But Dr. Goodnough says he has made it his cause to push for testing at least a month in advance of elective surgery, so that any problems can be treated well ahead of time and not cause you to cancel your procedure.
4. Anemia is more common with aging.
At least 8 percent of those over 65 suffer from anemia. This figure rises to 25 percent when people reach 75, a growing issue now that Americans are living longer. As many as half of anemia cases in the elderly are caused by either poor diet or kidney disease, both treatable conditions.
5. Chronic illness makes anemia more difficult to manage. Patients with cancer or kidney disorders face perhaps the hardest time, because both disease and treatment can make anemia worse. Women with cancer might suffer from three separate causes of fatigue, including the cancer, chemotherapy and blood loss from menstruating.
Normal Values:
Hemoglobin range Men : 13 - 18 Women : 12 - 17
Hematocrit range Men : 40 - 50 Women : 37 - 47
Tired Blood’ Warning: Ignore It at Your Peril
By Jane E. Brody : NY Times Article : July 19, 2008
Thanks to advertisements for the once-popular tonic Geritol, most people of a certain age know about “tired blood,” a disorder more accurately called anemia, involving a shortage of healthy red blood cells to carry oxygen to body tissues and cleanse them of carbon dioxide.
It is not really the blood of people with anemia that is “tired.” Rather, it is anemic people themselves who commonly experience chronic fatigue. Other symptoms may include weakness, shortness of breath, impaired athletic performance, rapid heartbeat, irritability, apathy, dizziness, pale skin, headache and numb or cold hands and feet. But in many people the symptoms are too mild to be recognized, and the anemia goes undetected for years.
Anemia is the most common blood disorder in the United States. Statistics indicate that 3.4 million Americans are anemic, but experts say that this is a gross underestimate and that anemia has been viewed for far too long as an “innocent bystander,” considered almost normal in certain groups, like menstruating women and the elderly.
But a growing body of research indicates that anemia can seriously compromise the quality of a person’s life, make sick people sicker and even speed deaths, said Dr. Allen Nissenson, a nephrologist and professor of medicine at the University of California, Los Angeles.
It is time to take anemia much more seriously, he added, making sure people have routine blood tests and are treated to restore healthy supplies of red blood cells. The testing is done either by a finger prick or by drawing blood from a vein. The finger test usually measures the hematocrit level, or percentage of red blood cells in plasma. A normal count is 36 percent to 46 percent for women and 46 percent to 56 percent for men.
A more accurate assessment measures the oxygen-carrying hemoglobin in blood, expressed as grams of hemoglobin per deciliter of blood. A normal hemoglobin for women is 12 to 13 grams, and for men, 13 to 14. Hemoglobin has traditionally been measured in blood from a vein, but a finger-prick test is now available.
Inadequate nutrition is the most common cause of anemia, Dr. Nissenson said. Production of hemoglobin, the oxygen-carrying protein on red blood cells, depends upon the mineral nutrient iron, most prominent in meat and poultry (especially organs like liver and kidneys) and egg yolks.
To a lesser degree, it is found in green leafy vegetables, dried fruits, dried beans and peas and enriched and whole grain cereals and bread. Foods rich in vitamin C help the body to absorb iron.
Also important to the production of healthy red cells are B vitamins, folic acid, B12 and B6. B12 occurs only in animal foods, especially meat, fish, eggs and milk. Dark green leafy vegetables are the best source of folic acid; whole grains are the best source of B6.
These nutrients are often in short supply among women who lose iron in menstrual blood, pregnant women, strict vegetarians, overly zealous dieters and poor people. Increasingly, the problem is found among elderly people on restricted diets.
Anemia afflicts virtually everyone with kidney disease because shrinking kidneys are not able to make enough of the hormone erythropoietin, which controls the production of red blood cells in the bone marrow. In addition, many chronic diseases involving inflammation can result in anemia, including congestive heart failure, inflammatory bowel disease, rheumatoid arthritis, AIDS, liver disease and cancer.
There are also hereditary anemias like sickle cell and thalassemia, and hemolytic anemias that involve the destruction of red blood cells faster than they can be replaced. Immune disorders and medicines can also bring it on.
Anemia can also result from chronic blood loss — from an ulcer, polyp or hemorrhoid — that may not be apparent without a stool test. Occasionally, a previously undetected cancer in the digestive tract can be the cause, so if no other responsible factor is identified, a colonoscopy should be done.
Doctors have long been aware of the risk of anemia in infants and in teenage girls and women of childbearing age, but anemia is far more prevalent in people over 65, studies say. One concluded that the incidence of anemia among the elderly was four to six times as great as had been suspected, affecting as many as a quarter of those over 75.
Even among patients with nearly identical medical disorders, those who are anemic tend to die faster. In one study of Medicare patients with congestive heart failure, for example, for every 1 percent decrease in the hematocrit (or percentage of red blood cells in plasma), the mortality rate rose by 1.6 percent.
In a study of nearly 79,000 elderly patients hospitalized with heart attacks, blood transfusions greatly lowered the death rate among those with hematocrits of less than 33 percent upon admission to the hospital.
Likewise with dialysis patients. In a study of 20,000 such patients with chronic kidney failure, those who were more severely anemic had a death rate twice that of patients less anemic. But when anemia in dialysis patients was treated effectively, the death rate after one year was no different from the rate in those who were not initially anemic.
Cancer patients also seem to do better when they are not anemic. Chemotherapy and radiation often cause anemia, which is associated with a reduced ability to control the disease and a lower survival rate.
Perhaps the most common consequence of anemia is an impaired quality of life, especially among older, ostensibly healthy people. In a study published in The American Journal of Medicine, Dr. Brenda W. J. H. Penninx and co-authors followed a group of 1,146 men and women 71 and older for more than four years.
The participants performed three tests at the start and end of the study: standing balance, a timed eight-foot walk and rising from a chair. Those with hemoglobin levels just slightly below normal were one and a half times as likely to experience physical declines as those with normal hemoglobin. Those with greater degrees of anemia experienced greater declines.
“Although no study yet shows that treating anemia in older people reduces the incidence of physical decline, our study certainly suggests that this may be the case,” Dr. Penninx said.
Anemia treatment is mainly determined by the cause: correcting underlying disorders, changing diets, adding nutritional supplements and for many, costly genetically engineered drugs like Procrit, Epogen and Aranesp.
Updated from an article that appeared in The Times on Sept. 23, 2003.
New Anemia Treatments Bring New Problems
By Eric Sabo : NY Times Article
Some forms of anemia, like those from nutritional deficiencies or bleeding, can be corrected by fixing the underlying problem. But anemia from cancer and chronic ailments like kidney disease are far more complex and can require years of specific treatment. Cancer patients, for example, face severe nausea and other side effects from chemotherapy, but they rate the tiredness from anemia as the most bothersome part of living with the disease.
Studies show that fatigued patients with anemia feel more energized after receiving transfusions of donated red blood cells, a procedure that has been around since the 16th century. But the process is laborious, and transfusions carry serious risks like emerging infectious diseases, mismatched blood types or fluid buildup in the lungs.
In recent years, doctors have found that newer anemia drugs like Procrit and Aranesp could produce roughly the same effects as transfusions, but with greater ease and seemingly less risk. The medications, which are also injected but in less time, made a lasting impact on many fatigued patients, who say they regained at least some of their old vigor when little else worked. Prescriptions for the drugs soared.
Yet the top-selling medications are undergoing a serious reappraisal after being linked to higher rates of heart attacks, stroke and early death. Early in 2008, the Food and Drug Administration’s scientific advisory board issued strict new warnings on the drugs, saying that higher than normal doses can lead to heart problems and also promote tumor growth in certain cancers. It was the second such warning that the F.D.A. had issued on the treatments in nearly a year.
“I think people need to be extremely cautious with the use of these drugs,” said Dr. Allen Nissenson of the University of California, Los Angeles. “At a minimum, patients should be satisfied with modest improvements from low doses as a way to minimize the risks.”
Dr. Douglas Rizzo, who directs the Center for International Blood and Marrow Transplant Research at the Medical College of Wisconsin, said it was still unclear whether high doses were at the root of the problem. The drugs stimulate production of erythropoietin, a hormone that helps blood cells ferry oxygen. But the natural energy booster also plays other roles in the body, including healing wounds, and making it a drug target could produce a range of unknown effects, he said.
“There’s a lot of uncertainty,” Dr. Rizzo said. “I think patients will have a difficult choice to make.”
And it’s not always a choice. A study published in The New England Journal of Medicine found that anemia drugs did not completely replace the use of transfusions in critically ill patients, so some people end up requiring both forms of treatment.
The only natural option, Dr. Nissenson said, is to move to higher ground. “It’s not a joke,” he said. Living at high altitude for a period of time stimulates the production of red blood cells to compensate for the lack of oxygen in mountainous areas.
“You don’t need to go to Mount Everest,” Dr. Nissenson said. “If you look at people in Denver, Colorado their average hemoglobin is significantly higher than people at sea level.”
The Challenges of Anemia: Defining It, and Living With It
By Eric Sabo : NY Times Article : July 19, 2008
Dr. Allen Nissenson is a professor of medicine and director of the dialysis program for the David Geffen School of Medicine at the University of California, Los Angeles. He has written two medical textbooks on kidney disease treatment and was president of the National Anemia Action Council, a patient advocacy group.
Q: Anemia can result from a wide range of diseases and conditions. What are the most prominent causes?
A: And then there’s cancer itself, or the side effects from treating cancer, that can cause anemia. Another prominent cause is deficiencies in erythropoietin, or Epo, a hormone that stimulates red blood cell production, which is almost entirely a problem in people with kidney disease.
Q: A lot of symptoms of anemia share the same characteristics as being overworked or just tired. How do you tell the difference between normal fatigue and anemia?
A: You really can’t. One of the dilemmas with anemia is that the symptoms are pretty ubiquitous: tiredness, weakness, some difficulty in thinking clearly. They’re all kind of vague.
So what we tell people is if you have these symptoms and they go on for a long time or seem to be interfering with your ability to function normally, then you should see your doctor. One of the things you need to get checked is your hemoglobin level — the protein that carries oxygen in red blood cells — to see if that’s part of the anemia.
Q: Is there a specific cutoff point of hemoglobin that indicates whether someone is anemic?
A: One of the challenges is defining what normal is, and there’s no uniform acceptance of normal hemoglobin levels. The one most doctors use is from the World Health Organization. A hemoglobin level below 13 for men and below 12 for women is considered anemic.
Q: Nutritional deficiencies are a common cause of anemia. Do these arise from a poor diet or underlying disease?
A: Bleeding is one of the most prominent causes of iron deficiency, because when you bleed you lose red blood cells that contain iron. But there still is a significant prevalence of nutritional iron deficiencies, which is much more common in pregnant women and children because of their diets.
Nutritional iron deficiency is the biggest cause of anemia worldwide, and it’s a problem is some segments of the United States. For folate or vitamin B12, it’s much less common to be deficient.
Q: How difficult is to live with anemia?
A: It’s very tough. One of the things we learned, however, is that the ability of the body to adapt is tremendous. Over time, even people with moderately severe anemia say, “You know, I really don’t feel that bad.”
Although people are fatigued or can’t do as much as they could before, they slowly adapt their lifestyle. Instead of walking to the grocery store once a week, they may go once a month and buy everything they need because they’re too tired to keep going back. There’s a lot of adaptation that takes place, but anemia can be very debilitating.
Q: Is anemia life-threatening?
A: The only life-threatening anemia is if you have massive hemorrhaging. But chronic anemia can be life-threatening indirectly in the sense that prolonged, severe anemia can cause the heart to enlarge and overwork, leading to heart failure. So through that mechanism, anemia can lead to serious morbidity or mortality.
Q: The Food and Drug Administration has issued warnings on three similar anemia drugs: Procrit, Aranasep and Epogen. How safe are these to use?
A: The studies that raised the red flags were either in cancer patients or in people with kidney disease, and they all showed something similar: if you attempt to correct the anemia completely back up to normal hemoglobin levels, that’s not a good idea. You start getting strokes or heart attacks, blood-clotting problems or increased mortality.
The recent studies that the F.D.A. flagged were just studies. Kidney specialists weren’t practicing this way — they were waiting for the studies. So we’re going to continue practicing the way we were, which is to give modest doses of the drugs, with modest improvements in hemoglobin.
Q: Are the drugs potentially dangerous for the elderly or other groups?
A: There are no studies to help us figure that out. There’s no question that since cancer patients and kidney patients are so different, but the same problem has arisen, I think people need to be extremely cautious with the use of these drugs.
One dilemma now is that if someone wanted to do a study on normalizing hemoglobin levels in the elderly with these drugs, I think an institutional review board that has to approve the ethics of studies like this would have a very difficult time because of the concerns of the risks.
Q: The F.D.A. says the drugs are safe to use in small doses that keep oxygen-carrying hemoglobin just below a level that is considered normal. Is this enough to help anemia patients feel better?
A: The quality of life benefit is seen with pretty modest increases of hemoglobin. It looks like you get the biggest bang for the buck early on. If you push the doses, then you start to see the toxicity.
Q: Are red blood cell transfusions a potentially safer option given the new concerns about the drugs?
A: As long as you’re aiming for a moderate increase in hemoglobin, the drugs are so much simpler and have few or any side effects unless you start pushing them hard. Whereas with transfusions, you still have the risk of infectious diseases and other issues.
Q: Are there lifestyle measures, like diet or exercise, that can treat anemia?
A: In the chronic conditions, there is probably very little that can be done. Obviously for nutritional anemia, improving nutrition will help. Probably the only thing you can do is to go to a higher altitude, because there’s less oxygen available.
As a result, the cells that make Epo detect that and then stimulate Epo to make more red blood cells. Even people with chronic illnesses have slightly higher hemoglobin when they go to altitude for a period of time.
What to Ask About Anemia
By Eric Sabo : NY Times Article : July 19, 2008
Confronting a new diagnosis can be frightening — and because research changes so often, confusing. Here are some questions you may not think to ask your doctor, along with notes on why they’re important.
How do I know if my fatigue is caused by anemia?
A physical exam will help determine the severity of your fatigue, along with other symptoms like weakness or difficulty concentrating. Doctors then test the level of hemoglobin in your blood, a substance that helps red blood cells carry oxygen to the body’s tissues, giving you strength. Persistent fatigue and lower than normal hemoglobin levels mean that you have anemia. Some doctors may also test your hematocrit level, which measures how much of your blood is made up of red blood cells. Low hematocrit is a further indication of anemia.
Can I get anemia from not eating properly?
Diets low in iron, vitamin B12 or folate can lead to anemia. But these nutrients are plentiful in most foods, and it does not take a significant amount of them to return nutrient levels to normal. Good sources of iron include red meats like liver, as well as poultry, fish, eggs, spinach and peas. The same types of animal products also contain B12, and most breakfast cereals are now specially fortified with the vitamin. Folate is a form of vitamin B found in breads, pasta and leafy vegetables.
Am I at risk for anemia if it runs in my family?
A small portion of anemias can be passed on to children at birth, namely thalassemias and sickle cell anemia. These are inherited genetic disorders that can cause the body to make fewer healthy red blood cells and less hemoglobin.
What diseases cause anemia?
Several chronic diseases can cause anemia, including rheumatoid arthritis and other inflammatory disorders that block the body’s ability to absorb iron. Virtually everyone with a long-term kidney disorder suffers from anemia because the kidneys are not able to make enough erythropoietin, which controls the production of red blood cells. Anemia is also prevalent in cancer patients, both from the disease and treatments like chemotherapy. People with heart disease or AIDS also often suffer from anemia.
How dangerous is anemia?
Anemia is not directly life-threatening unless it is linked to serious bleeding. But over time, anemia can cause the heart to overwork to compensate for the lack of energy. Patients with anemia tend to live shorter lives than those who suffer the same chronic diseases but without the fatigue.
Will anemia clear up over time?
Yes, as long as the underlying condition that caused the anemia is taken care of. Cancer patients who suffer from anemia, for example, may return to normal once their disease is in remission and treatment stops. Nutritional anemias are often easy to correct, with most people quickly returning to normal once they begin eating a proper diet.
Which anemia treatment should I use?
Iron supplements may be used if you are deficient in iron, either from a poor diet or chronic bleeding. The main treatment for many forms of anemia is using a drug to stimulate erythropoietin. The other major option is a red blood cell transfusion, which involves transferring donated oxygen-carrying blood cells to the anemic patient. Both treatments can improve symptoms of fatigue, but they are not a cure.
Are anemia drugs safe to use if I have cancer?
The Food and Drug Administration issued strict new precautions on anemia drugs after several studies found that higher-than-normal doses of the medications speeded tumor growth and shortened the lives of cancer patients. Those with breast cancer or cancers of the head and neck appear to have the highest risk and should consider forgoing the drugs altogether, a majority of experts convened by the F.D.A. recently advised.
In other tumor types, only patients receiving chemotherapy should take the drugs, because those who used anemia medications when they were not treating their cancer had higher rates of death. The F.D.A. recommends that cancer patients talk to their doctors about the risks and benefits of other options like red blood cell transfusions.
Are anemia drugs safe if I have kidney disease?
Many experts say that the benefits still outweigh the risks for people with kidney problems, as long as the drugs are used in moderate doses with modest aims. Studies have reported a higher number of deaths, nonfatal heart attacks, strokes and blood clots with high doses. The dangers appear to show up only after hemoglobin levels reach near-normal levels. Nearly everyone with kidney disease suffers anemia, and even modest improvements may restore some normalcy to people’s lives.
Are blood cell transfusions safe, and when should they be used?
Transfusions are routinely used to replace blood lost from serious injuries and during surgeries. They are also a common treatment for serious types of anemia, like sickle cell disease. But doctors consider transfusions a treatment of last resort for less severe anemia, because there is always a chance for spreading infectious disease and patients sometimes are matched with the wrong blood type. Better screening methods have significantly lowered these risks, but chronic anemia suffers may need several blood transfers, and the procedures are linked to greater problems the more they are used.
Can lifestyle measures treat anemia?
Nutritional anemias can be cleared up by getting more iron and vitamins. Researchers are studying whether exercise and special diets may increase energy in anemia patients, much like the benefits found in a range of other conditions. Living at higher altitude for a period of time is linked to naturally higher levels of hemoglobin and may help people feel less tired.
A: The biggest categories are nutritional anemias, which are mainly iron deficiency, but also deficiencies in folic acid or vitamin B12. Another major cause is bleeding, usually from the gastrointestinal tract. Chronic diseases that have an inflammatory component, like rheumatoid arthritis, can also cause anemia.
5 Things To Know Tips for Taking On Anemia
By Eric Sabo : NY Times Article : July 19, 2008
Dr. Lawrence Goodnough is the director of transfusion services at the Stanford University Medical Center and was president of the Society for the Advancement of Blood Management, a group that promotes better anemia control. He says that anemia is a serious medical condition, especially for people who suffer fatigue from chronic diseases. Here are the five things he believes everyone should know about managing the most common blood disorder.
1. Recognize the symptoms.
Headaches, dizziness, difficulty thinking and fatigue are the hallmarks of anemia. If these symptoms persist, see a doctor for a blood test. Having a low level of hemoglobin — the oxygen-carrying part of blood — can help determine if you suffer from anemia.
2. Take anemia seriously.
Everyone experiences fatigue from time to time, but anemia can sap your energy for long periods and keep you from doing the things you like. The symptoms may indicate an underlying bleeding problem that needs to be taken care of. Treatment for nutritional anemias can be as simple as getting more iron, vitamin B12 or folate, which are plentiful in most diets. More serious anemic conditions, like those caused by chronic diseases, may require special drugs or blood transfusions.
3. Get a blood test before surgery.
Doctors will test your hemoglobin levels a day or two before surgery because low levels could raise the risk of bleeding complications. But Dr. Goodnough says he has made it his cause to push for testing at least a month in advance of elective surgery, so that any problems can be treated well ahead of time and not cause you to cancel your procedure.
4. Anemia is more common with aging.
At least 8 percent of those over 65 suffer from anemia. This figure rises to 25 percent when people reach 75, a growing issue now that Americans are living longer. As many as half of anemia cases in the elderly are caused by either poor diet or kidney disease, both treatable conditions.
5. Chronic illness makes anemia more difficult to manage. Patients with cancer or kidney disorders face perhaps the hardest time, because both disease and treatment can make anemia worse. Women with cancer might suffer from three separate causes of fatigue, including the cancer, chemotherapy and blood loss from menstruating.
Sluggish? Confused? Vitamin B12 May Be Low
Melinda Beck : WSJ : January 18, 2011
Tired? Depressed? Forgetting things? Who isn't these days?
Those are also symptoms of a deficiency of B12, a key nutrient needed to make red blood cells and DNA and keep the nervous system working right.
Vitamin B12 deficiency is officially considered rare, affecting about 1 in 1,000 Americans, according to a 2005 study. But the incidence rises with age, to about 15% of elderly people. The rate is also much higher among people who don't eat meat or dairy products, people with absorption problems, people taking acid-blocking medications and those with Type 2 diabetes who take the drug Metformin.
"B12 deficiency is much more common than the textbooks and journal articles say it is," says Alan Pocinki, an internist in Washington D.C., who routinely tests his patients who fall into those categories. He also notes that since the Metformin connection was discovered only recently, some physicians aren't aware of it. "They assume that if patients complain of numbness and tingling in the feet, it's a diabetes issue and not a B12 issue."
Other symptoms of low B12 include anemia, depression, dementia, confusion, loss of appetite and balance problems. Long-term deficiency can bring severe anemia, nerve damage and neurological changes that may be irreversible.
Sometimes the symptoms are subtle. Internist Linda Assatourians, one of Dr. Pocinki's partners, says that a surprising number of her young female patients also have low levels of B12. Typically they are healthy and active, but they don't eat much meat and they have minor mood, memory or balance problems. "When I supplement their B12, they feel better," Dr. Assatourians says. "It's not a controlled study, but I see a lot of them."
"I was sort of tired, but I thought, 'It's winter and I'm doing too much,' " says Jessica Riester, 27, editor of publications for a German-American think tank. Her B12 level was slightly over 200 picograms per milliliter (the normal range is considered 200 to 800 pg per ml). After several weeks of B12 injections, then 1,000 milligrams daily in pill form, her B12 is now over 600 pg per ml and she says she feels better. "My color is better and the shadows under my eyes are gone," she says.
Indeed, several studies have shown that some symptoms of B12 deficiency, particularly early problems with cognitive function, can be apparent even when patients' blood levels are still in the normal range.
How Much
Recommended Dietary Allowances for vitamin B12 by age:
- 0-6 months: 400 nanograms
- 6-12 months: 500 ng
- 1-3 years: 900 ng
- 4-8 years: 1.2 micrograms
- 9-13 years: 1.8 mcg
- 14 years and older: 2.4 mcg
- Pregnant women: 2.6 mcg
- Nursing mothers: 2.8 mcg
Still, vitamin B12 isn't a miracle pick-me-up, a performance enhancer, a weight-loss aid or a quick way to sober up after a long night of drinking, as some celebrities and Internet marketers claim. For people who aren't deficient, "there's no evidence whatsoever that these injections are useful to pep you up," says Irwin H. Rosenberg, a professor and former dean of the Friedman School of Nutrition at Tufts University. Taking too much B12 is unlikely to be harmful, he adds; the excess is simply excreted.
B12 is one of the newest of the human vitamins, identified in 1948. It originates in bacteria, yeast and microbes in soil. Plants can't store it, so people get their B12 almost exclusively from meat, liver, poultry, fish and dairy products. Adults need just 2.4 micrograms a day, the amount in three ounces of beef, and can generally store it in fat tissue for several years. Dr. Pocinki speculates that some of his very lean patients are B12 deficient because they don't have much fat to store it in.
Some people have trouble absorbing B12 in the first place. Stomach acid is needed to release it from food particles. People who have used acid-blocking medications, particularly proton-pump inhibitors, for years may not have enough. And many elderly people naturally stop making stomach acid, so B12 deficiencies are increasingly common as people age.
Boosting B12
B12 comes almost exclusively from meat, liver, poultry, fish and dairy products. Some breakfast cereals are also fortified with the vitamin.
That's why the Institute of Medicine recommends that people over age 51 get most of their daily requirement from B12 supplements or cereals fortified with the vitamin that break down more easily in the digestive tract.
Further down the digestive tract, B12 must combine with a protein called intrinsic factor to be absorbed into the body. Without intrinsic factor, people absorb much less B12, resulting in a condition called pernicious anemia, in which red blood cells don't develop properly. Left untreated, pernicious anemia can bring on neurological changes, delusions and hallucinations. The discovery that eating large amounts of liver could cure pernicious anemia led to the Nobel Prize for medicine in 1934.
Other conditions can also interfere with B12 absorption, including celiac disease and Crohn's disease. "I thought I was going to die in my sleep because I had so little energy," says Ellen Icochea, a senior executive at the Federal Bureau of Investigation who had a very low B12 level along with several major medical problems. Weekly B12 injections made a dramatic difference. "It was like, 'Wow, here's energy!' " she says.
David H. Johnson, a 54-year old wildlife biologist, takes B12 shots every three days to cope with the challenges of chronic fatigue syndrome. "Imagine you are on a small roller coaster," he says. "You feel up one day and the next and then you start slumping until you're really flat again."
B12 comes in pill form and a new nasal spray, but injections are the fastest way to correct a severe deficiency, since it does not need to be absorbed in the digestive tract. Many patients learn to inject themselves or have a spouse do it to cut down on doctor visits. "I have world travelers who take their B12 and needles with them. It's like traveling with insulin," says Dr. Pocinki.
He says he has seen low-grade depression lift when patients were given B12 supplements.
Researchers are still investigating possible links between long-term B12 deficiency and other health problems. It's known, for example, that B12 and the other B vitamins help reduce homocysteine, an amino acid in the bloodstream that may be associated with heart disease. But several large prospective studies have not shown that taking B12 supplements reduces the risk.
It's also not clear whether low B12 raises the risk of dementia and Alzheimer's disease, although cognitive impairment brought on by low B12 is sometimes mistaken for Alzheimer's.
"It's really easy to miss, and really easy to fix," says Dr. Pocinki.
An additional concern: A high level of folic acid can mask symptoms of B12 deficiency, and many people are getting more folic acid than they realize. Since 1996, all enriched flour must contain folic acid to reduce the risk of neural-tube defects, a severe malformation that occurs in developing fetuses. Some studies suggest that having high folic acid can make cognitive damage from low B12 even worse.
"To this day, we are concerned about the trade-off," says Dr. Rosenberg, who was on the advisory panel that recommended enriching flour.
