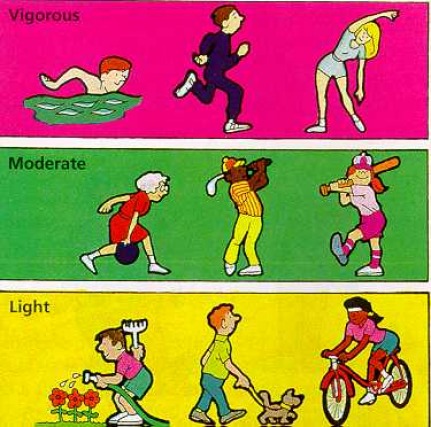
Exercise
Frequency : 3 - 5 times a week
· Intensity : Work out at 60% - 90% of your heart's maximum pumping capacity. Calculate by subtracting your age from 220 and then calculating 60% (for low intensity) - 90% (for high intensity) of this figure.
· Duration : 15 -60 minutes of continuous activity
· Mode : Any activity that involves large muscle groups in continuous movement eg running, walking, hiking, swimming, bicycling, rowing, rope skipping etc
Health Clubs & Gyms - Quick Tips
1.Before you join, think skeptically about what activities you are likely to participate in and how often you’ll be able to use the club. If you haven’t exercised before or for a long time, question whether you will be able to stick with a new fitness regimen. Most people who join clubs stop using them long before their memberships expire. Since most clubs charge nonrefundable initiation fees, and many clubs require or push annual contracts, you can waste a lot of money if you quit.
2.Consider whether you can get the exercise you want less expensively some other way—for example, by doing push-ups, sit-ups, and running on your own; by joining a sports team or exercise program; or by using a government-sponsored facility.
3.Shop. For roughly the same facilities, you might pay more than twice as much at some clubs as at others.
4.Be sure to press clubs you are considering for their best deals. When you are negotiating, get clubs to compete by mentioning other clubs you are considering. Many clubs have various fee plans and discount options and offer the best deals only if necessary to get the sale. Don’t allow sales staff to pressure you into making a decision. Check to see whether you qualify for a discounted rate due to an arrangement between your employer or health plan and the club. Find out about clubs’ rules on canceling a membership, selling a membership to someone else, and freezing a membership.
5.Try out any club you are considering by asking it for a guest pass to use. When you are there, check out the cleanliness and the condition of equipment, ask other members how crowded the club gets at hours when you might want to be there, and judge how helpful the staff is.
Stretching: The Truth
By Gretchen Reynolds : NY Times Article : November 2, 2008
When Duane Knudson, a professor of kinesiology at California State University, Chico, looks around campus at athletes warming up before practice, he sees one dangerous mistake after another. "They're stretching, touching their toes. . . . " He sighs. "It's discouraging."
If you're like most of us, you were taught the importance of warm-up exercises back in grade school, and you've likely continued with pretty much the same routine ever since. Science, however, has moved on. Researchers now believe that some of the more entrenched elements of many athletes' warm-up regimens are not only a waste of time but actually bad for you. The old presumption that holding a stretch for 20 to 30 seconds — known as static stretching — primes muscles for a workout is dead wrong. It actually weakens them. In a recent study conducted at the University of Nevada, Las Vegas, athletes generated less force from their leg muscles after static stretching than they did after not stretching at all. Other studies have found that this stretching decreases muscle strength by as much as 30 percent. Also, stretching one leg's muscles can reduce strength in the other leg as well, probably because the central nervous system rebels against the movements.
"There is a neuromuscular inhibitory response to static stretching," says Malachy McHugh, the director of research at the Nicholas Institute of Sports Medicine and Athletic Trauma at Lenox Hill Hospital in New York City. The straining muscle becomes less responsive and stays weakened for up to 30 minutes after stretching, which is not how an athlete wants to begin a workout.
THE RIGHT WARM-UP should do two things: loosen muscles and tendons to increase the range of motion of various joints, and literally warm up the body. When you're at rest, there's less blood flow to muscles and tendons, and they stiffen. "You need to make tissues and tendons compliant before beginning exercise," Knudson says.
A well-designed warm-up starts by increasing body heat and blood flow. Warm muscles and dilated blood vessels pull oxygen from the bloodstream more efficiently and use stored muscle fuel more effectively. They also withstand loads better. One significant if gruesome study found that the leg-muscle tissue of laboratory rabbits could be stretched farther before ripping if it had been electronically stimulated — that is, warmed up.
To raise the body's temperature, a warm-up must begin with aerobic activity, usually light jogging. Most coaches and athletes have known this for years. That's why tennis players run around the court four or five times before a match and marathoners stride in front of the starting line. But many athletes do this portion of their warm-up too intensely or too early. A 2002 study of collegiate volleyball players found that those who'd warmed up and then sat on the bench for 30 minutes had lower backs that were stiffer than they had been before the warm-up. And a number of recent studies have demonstrated that an overly vigorous aerobic warm-up simply makes you tired. Most experts advise starting your warm-up jog at about 40 percent of your maximum heart rate (a very easy pace) and progressing to about 60 percent. The aerobic warm-up should take only 5 to 10 minutes, with a 5-minute recovery. (Sprinters require longer warm-ups, because the loads exerted on their muscles are so extreme.) Then it's time for the most important and unorthodox part of a proper warm-up regimen, the Spider-Man and its counterparts.
"TOWARDS THE end of my playing career, in about 2000, I started seeing some of the other guys out on the court doing these strange things before a match and thinking, What in the world is that?" says Mark Merklein, 36, once a highly ranked tennis player and now a national coach for the United States Tennis Association. The players were lunging, kicking and occasionally skittering, spider-like, along the sidelines. They were early adopters of a new approach to stretching.
While static stretching is still almost universally practiced among amateur athletes — watch your child's soccer team next weekend — it doesn't improve the muscles' ability to perform with more power, physiologists now agree. "You may feel as if you're able to stretch farther after holding a stretch for 30 seconds," McHugh says, "so you think you've increased that muscle's readiness." But typically you've increased only your mental tolerance for the discomfort of the stretch. The muscle is actually weaker.
Stretching muscles while moving, on the other hand, a technique known as dynamic stretching or dynamic warm-ups, increases power, flexibility and range of motion. Muscles in motion don't experience that insidious inhibitory response. They instead get what McHugh calls "an excitatory message" to perform.
Dynamic stretching is at its most effective when it's relatively sports specific. "You need range-of-motion exercises that activate all of the joints and connective tissue that will be needed for the task ahead," says Terrence Mahon, a coach with Team Running USA, home to the Olympic marathoners Ryan Hall and Deena Kastor. For runners, an ideal warm-up might include squats, lunges and "form drills" like kicking your buttocks with your heels. Athletes who need to move rapidly in different directions, like soccer, tennis or basketball players, should do dynamic stretches that involve many parts of the body. "Spider-Man" is a particularly good drill: drop onto all fours and crawl the width of the court, as if you were climbing a wall. (For other dynamic stretches, see the sidebar below.)
Even golfers, notoriously nonchalant about warming up (a recent survey of 304 recreational golfers found that two-thirds seldom or never bother), would benefit from exerting themselves a bit before teeing off. In one 2004 study, golfers who did dynamic warm- up exercises and practice swings increased their clubhead speed and were projected to have dropped their handicaps by seven strokes over seven weeks.
Controversy remains about the extent to which dynamic warm-ups prevent injury. But studies have been increasingly clear that static stretching alone before exercise does little or nothing to help. The largest study has been done on military recruits; results showed that an almost equal number of subjects developed lower-limb injuries (shin splints, stress fractures, etc.), regardless of whether they had performed static stretches before training sessions. A major study published earlier this year by the Centers for Disease Control, on the other hand, found that knee injuries were cut nearly in half among female collegiate soccer players who followed a warm-up program that included both dynamic warm-up exercises and static stretching. (For a sample routine, visit www.aclprevent.com/pepprogram.htm.) And in golf, new research by Andrea Fradkin, an assistant professor of exercise science at Bloomsburg University of Pennsylvania, suggests that those who warm up are nine times less likely to be injured.
"It was eye-opening," says Fradkin, formerly a feckless golfer herself. "I used to not really warm up. I do now."
You're Getting Warmer: The Best Dynamic Stretches
These exercises- as taught by the United States Tennis Association's player-development program – are good for many athletes, even golfers. Do them immediately after your aerobic warm-up and as soon as possible before your workout.
STRAIGHT-LEG MARCH
(for the hamstrings and gluteus muscles)
Kick one leg straight out in front of you, with your toes flexed toward the sky. Reach your opposite arm to the upturned toes. Drop the leg and repeat with the opposite limbs. Continue the sequence for at least six or seven repetitions.
SCORPION
(for the lower back, hip flexors and gluteus muscles)
Lie on your stomach, with your arms outstretched and your feet flexed so that only your toes are touching the ground. Kick your right foot toward your left arm, then kick your leftfoot toward your right arm. Since this is an advanced exercise, begin slowly, and repeat up to 12 times.
HANDWALKS
(for the shoulders, core muscles, and hamstrings)
Stand straight, with your legs together. Bend over until both hands are flat on the ground. "Walk" with your hands forward until your back is almost extended. Keeping your legs straight, inch your feet toward your hands, then walk your hands forward again. Repeat five or six times. G.R.
Questions For Your Doctor : What to Ask About Exercise
By Marilynn Larkin : NY Times Article ; January 8, 2008
A new diagnosis can be a frightening experience, and ever-changing research can complicate already difficult treatment decisions. Here are some questions you might ask your doctor if exercise has been recommended as part of your treatment plan.
Why are you recommending exercise for my condition? I thought medication would be enough.
Physicians increasingly prescribe exercise as a complement to medication for a wide range of medical complaints, though it’s not a substitute for taking your drugs. Exercise may help slow progression of certain conditions, such as arthritis, Parkinson’s disease and chronic obstructive pulmonary disease, or improve other aspects of your health, including cardiovascular endurance and strength. Exercise can also boost mood and sense of well-being.
What kind of exercises should I do? Are there some I should avoid?
If you haven’t been exercising regularly, start by walking. And talk to your doctor first, especially if you’re over 50 or have a medical condition. He or she can recommend a physical therapist or other health professional with experience in your condition. A physical therapist can also show you how to add appropriate resistance and flexibility exercises to your routine.
Can medications affect my ability to exercise?
Some drugs may cause side effects like dizziness, so you want to be sure to choose exercises that allow you to stop and sit down if necessary. Other medications can affect heart rate, making it difficult to tell when you are exercising at or near your target heart rate.
Do I need to lose weight before I start?
Most people can embark on an exercise program regardless of weight. Begin by walking. If you can’t walk 30 minutes at a time, do shorter bouts. Exercising 10 minutes at a time, three times a day, confers similar benefits to exercising in a single 30-minute session, studies show. Increasing physical activity can also help minimize age-related weight gain.
I haven’t regularly exercised since college, and that was years ago. Can I really get benefits now?
You’re never too old to start, as the adage goes. In recent studies, people in their 70s and 80s demonstrated significant gains in strength and function from participation in a strength-training program. Older adults also get cardiovascular benefits from aerobic activity. Improving aerobic capacity and strength will make it easier to do everyday activities and allows older adults stay independent longer.
How do I get started?
Several Web-based programs can help you jump in, including the American Heart Association’s “Choose to Move” program and the “Exercise and Screening for You,” or EASY, tool from Texas A&M Health Science Center. Also see the American College of Sports Medicine’s brochure, Energy Expenditure in Different Modes of Exercise.
How much exercise should I do?
New exercise recommendations from the American College of Sports Medicine and the American Heart Association advise moderately intense aerobic exercise 30 minutes a day, five days a week, or vigorously intense aerobic exercise 20 minutes a day, three days a week. In addition, they recommend a mix of eight to 10 strength-training exercises -- on a schedule of 10 to 15 repetitions of each exercise two to three times per week for those with chronic ailments or people over 65.
Do I need to join a gym?
It’s not necessary to join a gym; all you need are a pair of athletic shoes and a little motivation. Some people find that exercising with a friend or in a group helps them stay on track.
Should I buy special equipment?
You don’t need special equipment. However, it may be helpful to invest in resistance bands or free weights to do resistance training. A stability ball to improve balance or a home exercise machine may also help. The American College of Sports Medicine offers brochures to help seniors and others make appropriate purchases and learn to use equipment properly.
I travel a lot for business. How can I keep up my exercise routine?
Know what fitness facilities are available at your hotel and in the immediate area. Plan exercise time around your business obligations. Be aware that the latest research suggests that you can take up to a week off from exercise without any significant reduction in your fitness level. During longer trips, focus on maintaining your fitness with some form of aerobic or strength training -- even though it might not be your usual routine --at least twice a week.
Post exercise recovery
By Gretchen Reynolds
NY Times Article : June 1, 2008
From the perspective of an athlete, few things top the virtuous satisfaction that comes from a hard workout. That 10-mile run, that 1,500-meter pool sprint, that hour with the free weights. Makes you feel great, right? You'll do it again tomorrow, for sure. But then it hits — the aftermath.
Within a few hours, your muscles begin sending vicious little reminders about your impressive efforts. Delayed-onset muscle soreness, as it's called, settles in roughly 12 to 24 hours after an intense bout of training, especially if it involved unfamiliar or extreme movements. The affected muscles become so tender and strained that the process of rising from bed the next morning becomes a challenge.
Even if you haven't arrived at this sorry state, repeated hard workouts can tax the body in insidious ways. Muscles, over the course of an hour or so of serious work, use up most of their stored energy. Without remediation, those muscles won't respond as well during your next workout. They'll be more prone to injury. You'll be slower. The 70-year-old from down the street will pass you on the running path.
Completing a hard workout, then, is just the first step. You also have to undo all the damage you've just done.
Start with your postworkout meal. The regeneration of your muscles begins, improbably as it may seem, with that. "Back in the early '90s, most athletes, especially runners and cyclists, were preoccupied with carbohydrates," says John Ivy, the chairman of the department of kinesiology and health education at the University of Texas in Austin and one of the pioneers of research into exercise recovery. This was in the heyday of carbo-loading, when athletes were convinced that the more pasta and bread they ate before a hard workout, the more stored energy they'd have.
But carbo-loading in advance of exercise is not the most efficient way to stock muscles with fuel, physiologists now know, thanks in large part to research conducted by Ivy. When reviewing studies of diabetics, he became intrigued by similarities with his own tests on cyclists: for both groups, insulin in the blood was more effective at carrying energy into the muscles if those muscles had recently been active. "Exercise makes your muscles more responsive to insulin, and this insulin, in turn, increases glycogen muscle uptake," he says. In other words, exercise prompts your muscles to absorb more fuel — glucose, which is stored as glycogen — from the bloodstream. (Carbo-loading can't take advantage of this insulin response because it precedes, rather than follows, a workout.) Your body is actually primed by the exercise to help itself replenish lost fuel.
This improved insulin response, however, lasts only for a brief time after a workout. "You have a window of about 30 to 45 minutes," Ivy says. After that, muscles become resistant to insulin and much less able to absorb glucose. Drinking or eating carbohydrates immediately after a strenuous workout, at a level of at least one gram per kilogram of body weight, is therefore essential to restoring the glycogen you've burned. Wait even a few hours and your ability to replenish that fuel drops by half.
It's also crucial that you take in some protein. Though it poses challenges to strict vegetarians, the latest research shows quite definitively that protein spurs even more of an insulin response than do exercise and carbohydrates alone. "Protein co-ingestion can accelerate muscle glycogen repletion by stimulating endogenous insulin release," says Luc van Loon, an associate professor of human movement sciences at Maastricht University in the Netherlands and the author of several important studies about recovery. Translation: coupling protein with carbohydrates prompts your muscles to store even more glycogen for use during your next workout.
"I'd advise people to have their recovery drink ready and waiting for them before they leave on a run or long bike ride," Ivy says. Ivy himself often drinks low-fat chocolate milk, but any food or drink that includes both carbohydrates and protein — a recovery drink, a smoothie, yogurt — will work.
Then have a real meal within two hours. "You can maintain increased insulin levels and accelerated rates of recovery for about four to six hours if you continue eating," Ivy says. Of course, you can also get by without such diet timing. "But you won't recover as well," Ivy continues. "You probably won't be able to work out as hard on a daily basis." The old guy who chugs his milk and Hershey's syrup will not only pass you — he'll lap you.
Meanwhile, there's the physical damage inside your muscles to consider. Skeletal muscle is a unique kind of tissue, made up of long, thin fibers composed of several different proteins. These proteins interlock like Legos inside fibrous compartments called sarcomeres. Sarcomeres can stretch, but only so far.
During certain kinds of movements, some sarcomeres are pulled past their tolerance. The proteins inside separate, resulting in micro-tears throughout your muscle tissue. After a few hours, this leads to inflammation, swelling, stiffness and pain. (Eccentric muscle contractions, which lengthen muscles, are the main culprit in delayed-onset muscle soreness. Concentric contractions, in which muscles shorten — the upward motion of a biceps curl, for instance — cause less damage. That's why running downhill makes you more sore the next day than running on flat ground.)
"This soreness is actually a good thing," says Thomas Swensen, a professor of exercise and sports science at Ithaca College in Ithaca, N.Y., and a leading researcher into exercise recovery. "You want to stress the muscles. They will adapt positively." The muscles will rebuild themselves, becoming stronger and more pliable. "That's the whole point of hard training," he says. "But it's only effective if you recover fully."
Which is another reason it's important to up your protein intake after a workout; that same protein will also help speed muscle repair. "Exercise stimulates muscle protein synthesis and protein breakdown," van Loon says. "However, without protein or amino acid ingestion, the net balance between protein synthesis and breakdown will remain negative" — i.e., your workouts, in the long run, may do your muscles more harm than good. But eat enough protein immediately after exercising and your muscles will repair themselves fully and become stronger.
Other postworkout recovery strategies, including many that athletes swear by, have far less scientific backing. Take massage. A 2000 study of British boxers showed that postworkout massage made the athletes only feel as if they were recovering quickly; they did not perform any better than those not massaged. Swensen's own 2003 study of massage and recovery produced similar results as the British research.
These studies, however, like many others that have examined massage and exercise, were small and short-term. "It's possible that if you followed athletes over the course of several months," Swensen says, "you might see some benefits from massage. Those studies haven't been done."
Similar ambiguity clouds the use of ibuprofen after exercise. Although advertised as an anti-inflammatory, ibuprofen doesn't always work as expected. A 2006 study of the drug's use among ultra-marathoners found that it did not lessen muscle damage or soreness or reduce inflammation. And although most users do not experience side effects, ibuprofen has been associated with kidney damage and gastrointestinal bleeding.
Finally, there are ice and heat. Many elite athletes swear by a limb-numbing ice bath, and others prefer a soak in a hot tub — although little scientific evidence supports either remedy. Ice will effectively block the swelling associated with a serious injury, such as a sprain, but has not been proven to speed the healing of muscle tissue stressed by a workout. In a study published last year in the British Journal of Sports Medicine, people treated with ice after strenuous exercise later reported more pain upon standing than people immersed in tepid water. The study's authors bluntly concluded that their research "challenges the wide use of [icing] as a recovery strategy by athletes." Similarly, a study published in March in the European Journal of Applied Physiology found that, when it came to muscle recovery, a hot bath was little better than merely sitting quietly for a while.
So where does that leave you, the athlete who has just worked out so diligently? Mixing a smoothie or glass of chocolate milk, the one recovery strategy that satisfies both your inner physiologist and inner child. .
Exercise
Exercise for life.
Before you start an exercise program
If you have decided to start an exercise program, you are already on your way to a healthier heart and a fitter body. The first step you should take is to see your doctor, especially if you have any of the health risks listed below:
There are 3 categories of exercises: cardiovascular, strength-building, and flexibility.
Cardiovascular exercise is also known as aerobic exercise. Aerobic exercise uses your large muscles and can be continued for long periods. For example, walking, jogging, swimming, and cycling are aerobic activities. These types of exercises drive your body to use oxygen more efficiently and deliver maximum benefits to your heart, lungs, and circulatory system.
Strength-building and flexibility exercises are known as anaerobic exercise. Anaerobic exercise does not have cardiovascular benefits, but it makes your muscles and bones stronger. Strength-building exercises require short, intense effort. Flexibility exercises, which are also anaerobic, tone your muscles through stretching and can prevent muscle and joint problems later in life.
A well-balanced exercise program should include some type of exercise from each category.
Cardiovascular Exercise
A simple definition of cardiovascular exercise is any exercise that raises your heart rate to a level where you can still talk, but you start to sweat a little.
At least 20 minutes of cardiovascular exercise 3 or 4 days a week should be enough to maintain a good fitness level. Any movement is good, even house or yard work. But if your goal is to lose weight, you will need to do some form of cardiovascular exercise for 4 or more days a week for 30 to 45 minutes or longer.
The ideal cardiovascular exercise program starts with a 5- to 10-minute warm-up, which includes gentle movements that will slightly increase your heart rate.
Then, slowly move into 20 or more minutes of a cardiovascular exercise of your choice, such as aerobics, jogging on a treadmill, or walking, to reach what is called your target heart rate. (The chart below can help you find your target heart rate zone.) Your target heart rate is a guideline that can help you measure your fitness level before the start of your program and help you keep track of your progress after you begin an exercise program. Target heart rate also lets you know how hard you are exercising. If you are beginning an exercise program, you should aim for the low end of your target heart rate zone. If you exercise regularly, you may want to work out at the high end of the zone.
To stay within your target heart rate zone, you will need to take your pulse every so often as you exercise. You can find your pulse in 2 places: at the base of your thumb on either hand (called the radial pulse), or at the side of your neck (called the carotid pulse). Put your first 2 fingers over your pulse and count the number of beats within a 10-second period. Multiply this number by 6, and you will have the number of heartbeats in a minute. For example, if you counted your pulse to be 20 during the 10-second pulse count, your heart rate would be 120 beats per minute.
Note: If you are taking certain medicines, like beta blockers, you may not be able to reach your target heart rate. Remember, always have your doctor's approval before beginning any exercise program.
You never want to begin exercising by immediately reaching your target heart rate, because your muscles and circulatory system need to warm up slowly. Intensify your activity slowly during exercise until you reach your target heart rate. There is no need to exceed your target heart rate during exercise.
End your exercise program with a 5- to 10-minute cool down, which will help to lower your heart rate and prevent your muscles from tightening up.
Strength-Building Exercise
People who lift weights or who use any type of equipment that requires weights are doing strength-building exercise. Strength-building exercise makes your muscles and bones stronger and increases your metabolism. Strength exercises also make your muscles larger. Your muscles use calories for energy even when your body is at rest. So, by increasing your muscle mass, you are burning more calories all of the time. If you strength train regularly, you will find that your body looks leaner and you will lose fat.
Strength-building exercises should be performed 2 to 3 times a week for best results. Always warm up your muscles for 5 to 10 minutes before you begin lifting any type of weight or before performing any resistance exercises.
Find a weight that you can comfortably lift for between 8 and 12 repetitions (reps). Reps are the number of times the exercise is performed. When you can easily do 12 to 15 reps of an exercise, it is time to increase the amount of weight you are lifting.
You should choose exercises that work your legs, arms, chest, back, and stomach. Make sure that each movement is performed in a slow, controlled way. Do not jerk the weights or use too much force.
Also, do not hold your breath during the movements. Remember to breathe out as you lift the weight and breathe in as you lower the weight.
Flexibility Exercises
Flexibility exercises are the most neglected part of a fitness program. Having flexibility can improve your posture, reduce your risk of injury, give you more freedom of movement, and release muscle tension and soreness.
Before you start the stretching phase of your program, always do 5 to 10 minutes of warm-up to loosen your muscles. Stretching cold muscles can lead to injury. Some examples of a warm-up are walking around, marching in place, slowly riding an exercise bike, or lightly jogging. If stretching is part of a longer program that includes a cardiovascular workout, always stretch after the cool-down section of your program. You want to make sure that your heart rate has slowed before you begin the stretching phase.
You should try to do stretching exercises for each muscle group. Each stretch should be done slowly and held for at least 10 to 30 seconds.
Do not bounce while you stretch, because bouncing can injure your muscles. Also, do not over stretch a muscle, because it can cause strain or even a tear. Try not to hold your breath while you stretch. Instead, take long, deep breaths throughout your stretching program.
Choosing the right program
Whether you decide to join a health club or to exercise on your own, you will make exercise a regular part of your life if you like doing it. So try to find one or more activities that you like to do or that give you satisfaction. Remember that exercise does not have to feel like a strenuous workout. Your body benefits from any type of movement. So if running or weight lifting are not for you, think about an activity like tai chi or yoga.
If you decide to join a group exercise program like an aerobics class or water-fitness class, here are some tips for choosing a program:
Preventing exercise injuries
One of the most important parts of an exercise program is the warm-up, but most people do not take the time to warm up properly.
A warm up increases your body temperature and makes your muscles loose and ready to exercise. Marching in place, walking for a few minutes, doing some jumping jacks, or jogging in place are all ways to get the blood flowing to the muscles and to prepare them for exercise.
These same exercises can and should be done to cool down after you exercise.
Buying good shoes before you begin an exercise program is one of the most important ways to make sure that you do not get hurt. Your shoes not only protect your feet but also give you a cushion for the weight of your whole body. That is why it is so important that your shoes fit properly.
You should go shoe shopping at the end of the day, when your foot is at its largest size. When you try on a shoe, there should be one-half inch between the end of your toe and the end of the shoe, and your foot should not slip or slide around inside.
Your shoes should feel good when you buy them, and they should not need a "breaking-in" period. If you are exercising regularly, you will most likely need to buy new shoes about every 3 to 6 months. Shoes that are used regularly lose the ability to absorb your weight during exercise and may cause injury to your knees and ankles.
If you are new to an exercise program, and you are exercising at a health club or fitness facility, ask for help before you try something new. The staff should be able to show you how to work any exercise equipment that you do not know how to use. Asking for help will stop you from lifting too much weight or from using the wrong posture when you use the machine. This, in turn, leads to fewer injuries.
Finally, use your good judgment and stay within your exercise limits. Light exercise performed regularly is always better than one gut-wrenching workout session a week. Your body will tell you if you are pushing it too hard. Pain, dizziness, fainting, a cold sweat, or pale skin are signs to stop. Even professional athletes and coaches will tell you that physical fitness is gained a little at a time.
Remember that exercise is not limited to working out in a health club or jogging around a track. Pushing a lawn mower, putting up storm windows, and vacuuming a rug are all forms of exercise, although they are not cardiovascular exercise. If you do not have a job that requires physical activity, taking the stairs instead of the elevator, parking farther away from your office, or taking a brief walk at lunch are all ways to find fitness during your day.
Exercise...Exercise....Exercise
By Jane E. Brody : NY Times Article : December 19, 2006
An apology to all baby boomers and beyond: I’m afraid that in our efforts to get everyone to become physically active, we’ve sold you a bill of goods. A 30-minute walk on most days is just not enough. There is much more to becoming — and staying — physically fit as you age than engaging in regular aerobic activity. (Of course, the same applies to those younger than 60.)
In addition to activities like walking, jogging, cycling and swimming that promote endurance, cardiovascular health and weight control, there is a dire need for exercises that improve posture and increase strength, flexibility and balance. These exercises can greatly reduce the risk of injuries from sports and endurance activities, the demands of daily life, falls and other accidents.
Musculoskeletal injuries are now the No. 1 one reason for seeking medical care in the United States. And falls, the Centers for Disease Control and Prevention reported last month, have become the leading cause of injury deaths for men and women 65 and older.
Unless you do something to slow the deterioration in muscle, bone strength and agility that naturally accompanies aging, you will become a prime candidate for what Dr. Nicholas A. DiNubile, an orthopedic surgeon at the Hospital of the University of Pennsylvania, calls “boomeritis.”
“By their 40th birthday, people often have vulnerabilities — weak links — and as the first generation that is trying to stay active in droves, baby boomers are pushing their frames to the breakpoint,” Dr. DiNubile said in introducing a November press event in New York sponsored by the American Academy of Orthopedic Surgeons and the National Athletic Trainers’ Association.
“Baby boomers are falling apart — developing tendinitis, bursitis, arthritis and ‘fix-me-itis,’ the idea that modern medicine can fix anything,” he said. “It’s much better to prevent things than to have to try to fix them.”
Dr. DiNubile pointed out that evolution had not kept up with the doubling of the human life span in the last 100 years. To counter the inevitable declines with age, we have to provide our bodies with an extended warranty.
Assess Your Fitness
In their recently published book, “Age-Defying Fitness” (Peachtree Publishers), two prominent physical therapists, Marilyn Moffat of New York University and Carole B. Lewis of Washington, D.C., provide the ingredients to help you make the most of your body for the rest of your life: a quick quiz and a five-part test to assess the status of your posture, strength, balance, flexibility and endurance, followed by five chapters with step-by-step instructions on how to safely improve the areas in which you are lacking.
The therapists describe what happens to these “five domains of fitness” as you age. Posture begins changing as early as the teenage years, the result of activities like prolonged sitting, carrying a heavy purse or briefcase, or working at a computer.
Strength declines as muscle fibers decrease in size and number and as the supply of nerve stimulation and energy to the muscles diminishes. Balance deteriorates as muscles tighten and weaken and joints lose their full range of motion.
Flexibility declines because connective tissue throughout the body becomes less elastic. And endurance falls off because of reduced flexibility, weakened muscles, and stiffer lungs and blood vessels.
Still not convinced you need to work on your fitness? See how you do on the therapists’ quiz:
“The antidote to aging is activity,” the therapists wrote. “Inactivity magnifies age-related changes, but action maintains and increases your abilities in all five domains.”
No Time to Waste
Dr. Vonda J. Wright, a sports medicine specialist at the University of Pittsburgh Medical Center, said at the New York meeting that “boomers are 59, and we must intervene now to head off what happens to those who age in a sedentary way.”
Injury and arthritis are the main reasons people stop exercising, she said. She urged those in need of a joint replacement not to postpone the surgery, which she likened to repairing a pothole.
Marjorie J. Albohm, a certified athletic trainer affiliated with OrthoIndy and the Indiana Orthopedic Hospital in Indianapolis, cautioned against “cookbook recipes” for exercise. “The key to a good workout is customization,” based on a professional assessment of flexibility, cardiovascular endurance, strength and balance, she said. “The goal is to minimize symptoms and prevent new injuries,” Ms. Albohm said, and she urged people to listen to their bodies to avoid making things worse.
Ms. Albohm emphasized flexibility, saying it is “not optional” as you age. “To prevent stiffness and maintain joint mobility you should stretch daily for 15 to 20 minutes,” she said “using slow, controlled movements, before or after your exercise program.”
For cardiovascular endurance, she recommended alternating between weight-bearing (walking, jogging) and non-weight-bearing (swimming, cycling) aerobic activities three days a week for 30 to 45 minutes each time.
Muscle strength, Ms. Albohm noted, can be increased at any age, even in one’s 90s, to protect against falls, maintain mobility, prevent new injuries and empower individuals. Especially important is strengthening the muscles in the front and sides of the thighs, which help support the knees, and strengthening core muscles of the trunk (back, buttocks and abdomen) to protect the spine and support the entire body.
Finally, we need to worry about our bones. At least 1.5 million “fragility fractures” occur annually in the United States. These are breaks that result when someone falls from a standing height or less, trips over the cat or lifts something heavy, and they affect men as well as women, Dr. Laura Tosi, an orthopedic surgeon at Children’s National Medical Center in Washington, D.C., said at the New York event.
“A history of a fragility fracture is far more predictive of future fractures than a bone density test,” Dr. Tosi said, adding that a major cause is a shortage of vitamin D, which lets calcium into bones.
“The current standard for vitamin D is not adequate,” she said, and predicted it would soon be raised to perhaps 1,000 International Units a day. Vitamin supplements are crucial, because adequate amounts of vitamin D cannot be absorbed through diet and sunshine alone.
Personal Health: You Name It and Exercise Helps It
By Jane E. Brody
NY Times Article : April 28, 2008
Randi considers the Y.M.C.A. her lifeline, especially the pool. Randi weighs more than 300 pounds and has borderline diabetes, but she controls her blood sugar and keeps her bright outlook on life by swimming every day for about 45 minutes.
Randi overcame any self-consciousness about her weight for the sake of her health, and those who swim with her and share the open locker room are proud of her. If only the millions of others beset with chronic health problems recognized the inestimable value to their physical and emotional well-being of regular physical exercise.
“The single thing that comes close to a magic bullet, in terms of its strong and universal benefits, is exercise,” Frank Hu, epidemiologist at the Harvard School of Public Health, said in the Harvard Magazine.
I have written often about the protective roles of exercise. It can lower the risk of heart attack, stroke, hypertension, diabetes, obesity, depression, dementia, osteoporosis, gallstones, diverticulitis, falls, erectile dysfunction, peripheral vascular disease and 12 kinds of cancer.
But what if you already have one of these conditions? Or an ailment like rheumatoid arthritis, multiple sclerosis, Parkinson’s disease, congestive heart failure or osteoarthritis? How can you exercise if you’re always tired or in pain or have trouble breathing? Can exercise really help?
You bet it can. Marilyn Moffat, a professor of physical therapy at New York University and co-author with Carole B. Lewis of “Age-Defying Fitness” (Peachtree, 2006), conducts workshops for physical therapists around the country and abroad, demonstrating how people with chronic health problems can improve their health and quality of life by learning how to exercise safely.
Up and Moving
“The data show that regular moderate exercise increases your ability to battle the effects of disease,” Dr. Moffat said in an interview. “It has a positive effect on both physical and mental well-being. The goal is to do as much physical activity as your body lets you do, and rest when you need to rest.”
In years past, doctors were afraid to let heart patients exercise. When my father had a heart attack in 1968, he was kept sedentary for six weeks. Now, heart attack patients are in bed barely half a day before they are up and moving, Dr. Moffat said.
The core of cardiac rehab is a progressive exercise program to increase the ability of the heart to pump oxygen- and nutrient-rich blood more effectively throughout the body. The outcome is better endurance, greater ability to enjoy life and decreased mortality.
The same goes for patients with congestive heart failure. “Heart failure patients as old as 91 can increase their oxygen consumption significantly,” Dr. Moffat said.
Aerobic exercise lowers blood pressure in people with hypertension, and it improves peripheral circulation in people who develop cramping leg pains when they walk — a condition called intermittent claudication. The treatment for it, in fact, is to walk a little farther each day.
In people who have had transient ischemic attacks, or ministrokes, “gradually increasing exercise improves blood flow to the brain and may diminish the risk of a full-blown stroke,” Dr. Moffat said. And aerobic and strength exercises have been shown to improve endurance, walking speed and the ability to perform tasks of daily living up to six years after a stroke.
As Randi knows, moderate exercise cuts the risk of developing diabetes. And for those with diabetes, exercise improves glucose tolerance — less medication is needed to control blood sugar — and reduces the risk of life-threatening complications.
Perhaps the most immediate benefits are reaped by people with joint and neuromuscular disorders. Without exercise, those at risk of osteoarthritis become crippled by stiff, deteriorated joints. But exercise that increases strength and aerobic capacity can reduce pain, depression and anxiety and improve function, balance and quality of life.
Likewise for people with rheumatoid arthritis. “The less they do, the worse things get,” Dr. Moffat said. “The more their joints move, the better.”
Exercise that builds gradually and protects inflamed joints can diminish pain, fatigue, morning stiffness, depression and anxiety, she said, and improve strength, walking speed and activity.
Exercise is crucial to improving function of total hip or knee replacements. But “most patients with knee replacements don’t get intensive enough activity,” Dr. Moffat said.
Water exercises are particularly helpful for people with multiple sclerosis, who must avoid overheating. And for those with Parkinson’s, resistance training and aerobic exercise can increase their ability to function independently and improve their balance, stride length, walking speed and mood.
Resistance training, along with aerobic exercise, is especially helpful for people with chronic obstructive pulmonary disease; it helps counter the loss of muscle mass and strength from lack of oxygen.
In the February/March issue of ACE Certified News, Natalie Digate Muth, a registered dietitian and personal trainer, emphasized the value of a good workout for people suffering from depression. Mastering a new skill increases their sense of worth, social contact improves mood, and the endorphins released during exercise improve well-being.
“Exercise is an important adjunct to pharmacological therapy, and it does not matter how severe the depression — exercise works equally well for people with moderate or severe depression,” wrote Ms. Muth, who is pursuing a medical degree at the University of North Carolina, Chapel Hill.
Feel-Good Hormones
Healthy people may have difficulty appreciating the burdens faced by those with chronic ailments, Dr. Nancey Trevanian Tsai noted in the same issue of ACE Certified News. “Oftentimes, disease-ridden statements — like ‘I’m a diabetic’ — become barricades that keep clients from seeing themselves getting better,” she said, and many feel “enslaved by their diseases and treatments.”
But the feel-good hormones released through exercise can help sustain activity.
“With regular exercise, the body seeks to continue staying active,” wrote Dr. Tsai, an assistant professor of neurosciences at the Medical University of South Carolina in Charleston. She recommended an exercise program tailored to the person’s current abilities, daily needs, medication schedule, side effects and response to treatment.
She urged trainers who work with people with chronic ailments to start slowly with easily achievable goals, build gradually on each accomplishment and focus on functional gains. Over time, a sense of accomplishment, better sleep, less pain and enhanced satisfaction with life can become further reasons to pursue physical activity.
“Even if exercise is tough to schedule,” Dr. Moffat said, “you feel so much better, it’s crazy not to do it.”
Rest and Motion. The value of interval training
By Peter Jaret : NY Times article : May 3, 2007
Some gym goers are tortoises. They prefer to take their sweet time, leisurely pedaling or ambling along on a treadmill. Others are hares, impatiently racing through miles at high intensity.
Each approach offers similar health benefits: lower risk of heart disease, protection against Type 2 diabetes, and weight loss.
But new findings suggest that for at least one workout a week it pays to be both tortoise and hare — alternating short bursts of high-intensity exercise with easy-does-it recovery.
Weight watchers, prediabetics and those who simply want to increase their fitness all stand to gain.
This alternating fast-slow technique, called interval training, is hardly new. For decades, serious athletes have used it to improve performance.
But new evidence suggests that a workout with steep peaks and valleys can dramatically improve cardiovascular fitness and raise the body’s potential to burn fat.
Best of all, the benefits become evident in a matter of weeks.
“There’s definitely renewed interest in interval training,” said Ed Coyle, the director of the human performance laboratory at the University of Texas at Austin.
A 2005 study published in the Journal of Applied Physiology found that after just two weeks of interval training, six of the eight college-age men and women doubled their endurance, or the amount of time they could ride a bicycle at moderate intensity before exhaustion.
Eight volunteers in a control group, who did not do any interval training, showed no improvement in endurance.
Researchers at McMaster University in Hamilton, Ontario, had the exercisers sprint for 30 seconds, then either stop or pedal gently for four minutes.
Such a stark improvement in endurance after 15 minutes of intense cycling spread over two weeks was all the more surprising because the volunteers were already reasonably fit. They jogged, biked or did aerobic exercise two to three times a week.
Doing bursts of hard exercise not only improves cardiovascular fitness but also the body’s ability to burn fat, even during low- or moderate-intensity workouts, according to a study published this month, also in the Journal of Applied Physiology. Eight women in their early 20s cycled for 10 sets of four minutes of hard riding, followed by two minutes of rest. Over two weeks, they completed seven interval workouts.
After interval training, the amount of fat burned in an hour of continuous moderate cycling increased by 36 percent, said Jason L. Talanian, the lead author of the study and an exercise scientist at the University of Guelph in Ontario. Cardiovascular fitness — the ability of the heart and lungs to supply oxygen to working muscles — improved by 13 percent.
It didn’t matter how fit the subjects were before. Borderline sedentary subjects and the college athletes had similar increases in fitness and fat burning. “Even when interval training was added on top of other exercise they were doing, they still saw a significant improvement,” Mr. Talanian said.
That said, this was a small study that lacked a control group, so more research would be needed to confirm that interval training was responsible.
Interval training isn’t for everyone. “Pushing your heart rate up very high with intensive interval training can put a strain on the cardiovascular system, provoking a heart attack or stroke in people at risk,” said Walter R. Thompson, professor of exercise science at Georgia State University in Atlanta.
For anyone with heart disease or high blood pressure — or who has joint problems such as arthritis or is older than 60 — experts say to consult a doctor before starting interval training.
Still, anyone in good health might consider doing interval training once or twice a week. Joggers can alternate walking and sprints. Swimmers can complete a couple of fast laps, then four more slowly.
There is no single accepted formula for the ratio between hard work and a moderate pace or resting. In fact, many coaches recommend varying the duration of activity and rest.
But some guidelines apply. The high-intensity phase should be long and strenuous enough that a person is out of breath — typically one to four minutes of exercise at 80 to 85 percent of their maximum heart rate. Recovery periods should not last long enough for their pulse to return to its resting rate.
Also people should remember to adequately warm up before the first interval. Coaches advise that, ideally, people should not do interval work on consecutive days. More than 24 hours between such taxing sessions will allow the body to recover and help them avoid burnout.
What is so special about interval training? One advantage is that it allows exercisers to spend more time doing high-intensity activity than they could in a single sustained effort. “The rest period in interval training gives the body time to remove some of the waste products of working muscles,” said Barry A. Franklin, the director of the cardiac rehabilitation and exercise laboratories at the William Beaumont Hospital in Royal Oak, Mich.
To go hard, the body must use new muscle fibers. Once these recent recruits are trained, they are available to burn fuel even during easy-does-it workouts. “Any form of exercise that recruits new muscle fibers is going to enhance the body’s ability to metabolize carbohydrates and fat,” Dr. Coyle said.
Interval training also stimulates change in mitochondria, where fuel is converted to energy, causing them to burn fat first — even during low- and moderate-intensity workouts, Mr. Talanian said.
Improved fat burning means endurance athletes can go further before tapping into carbohydrate stores. It is also welcome news to anyone trying to lose weight or avoid gaining it.
Unfortunately, many people aren’t active enough to keep muscles healthy. At the sedentary extreme, one result can be what Dr. Coyle calls “metabolic stalling” — carbohydrates in the form of blood glucose and fat particles in the form of triglycerides sit in the blood. That, he suspects, could be a contributing factor to metabolic syndrome, the combination of obesity, insulin resistance, high cholesterol and elevated triglycerides that increases the risk of heart disease and diabetes.
The Benefits of lifting weights
By Judy Foreman : Boston Globe Article : January 21, 2008
I'm an exercise junkie - and proud of it. I swim, I run, I bike.
But, like many other people, I'm a disaster when it comes to lifting weights, also called strength, or resistance, training. The closest I come is lifting a few tiny dumbbells at home in front of the TV. And that's only when the Red Sox are on.
This is about to change, and not just because of lingering New Year's resolutions.
A growing body of evidence shows that strength training not only provides many benefits that aerobic workouts alone cannot, but also offers some of the same health benefits as aerobic conditioning.
It's long been known that weight lifting becomes more important as you get older to prevent injury and preserve the strength to do normal things like climbing stairs, hauling groceries, and chasing grandchildren.
What's comparatively new is that it does much more than that, potentially reducing the risk of developing heart disease, relieving neck pain, improving balance, and making it easier to battle the bulge - though it needs to be done properly to avoid injury.
The evidence for the value of strength training has grown so much that last year, the American College of Sports Medicine and the American Heart Association issued new recommendations for healthy adults 65 and older that stressed the importance of weight lifting.
The groups now recommend that all older Americans do eight to 10 repetitions for each of the major muscle groups (biceps, quadriceps, hamstrings, etc.). Resistance exercises should be done on two or more nonconsecutive days of the week.
The idea is to lift a weight that's heavy enough to work each muscle group until it is fatigued, so the amount you lift will increase as your strength grows. Weight-bearing exercise, like walking or running, does not count as weight lifting - that means you really have to lift weights or work out on a resistance machine.
One of the biggest benefits of strength training is that it dramatically increases muscle mass, which aerobic exercise does not, noted William J. Evans, director of the Nutrition, Metabolism, and Exercise Laboratory at the University of Arkansas for Medical Sciences. More muscle mass is good not just because it makes you stronger but because it increases basal metabolic rate - muscle cells even at rest burn more calories than fat cells.
Moreover, while aerobic exercise can significantly, although temporarily, increase blood pressure, a potential concern for some heart patients, resistance training does so only minimally, Evans said. Weight training also gets results fast - it only takes resistance training twice a week for a few weeks to begin to see a significant effect, compared with three days a week with aerobics.
Indeed, the more researchers probe the benefits of weight training for specific conditions, the stronger the case they can make, said Miriam Nelson, director of the John Hancock Center for Physical Activity and Nutrition at Tufts University.
Although studies have not yet proven that strength training lowers the risk of osteoporosis, Nelson said, they do show it lowers the risk of fractures by improving balance, bone density, and muscle mass. Weight training is also good for people with arthritis, she said, because stronger muscles can take the pressure off inflamed joints.
Weight training has been shown to have other benefits, too.
Research by Steven N. Blair, an exercise scientist at the University of South Carolina, suggests that people with greater muscle strength may be somewhat less likely to develop metabolic syndrome, a cluster of factors that raise the risk of heart disease and diabetes, such as increased waist size, high fasting blood sugar, high triglycerides, low HDL or "good" cholesterol, and high blood pressure. More studies are needed to confirm this association.
For older people with physical disabilities, 66 trials reviewed by Cochrane Collaboration, an international nonprofit group that evaluates health treatments, increasing strength and, to a lesser extent, function. A different 2007 Cochrane review of 34 studies showed that exercises, including strength training, can improve balance in women age 75 and older. Yet another 2007 Cochrane review of 34 studies on fibromyalgia (musculoskeletal pain) showed strength training may improve physical capacity.
And a Danish study just published last week showed that strength training can diminish the chronic neck pain of at computers.
I could go on. But I'm convinced. Weight training may not be as much fun as a run in the park. But I need it. I'm guessing you do, too.
The value of resistance training and the heart
While conventional wisdom once held that people with heart disease should not pump iron, a new scientific statement from the American Heart Association says some resistance training can be good for them.
"Just like we once learned that people with heart disease benefited from aerobic exercise, we are now learning that guided, moderate weight training also has significant benefits," said Mark Williams, professor of medicine at Creighton University School of Medicine in Omaha, Nebraska.
Weight training is seen as a complement to aerobic exercise, not a replacement, he said. But it provides everyday benefits.
"It helps people better perform tasks of daily living -- like lifting sacks of groceries," Williams said in a statement.
Resistance training is not recommended for people with certain conditions such as unstable heart disease, uncontrolled high blood pressure or heart rhythm disorders, infections in and around the heart, and some other serious problems.
The statement's recommendations for an initial weight-lifting program says resistance training should be performed:
And they are easier to stick to.
"For people with cardiovascular disease, the level of resistance should be reduced and number of repetitions increased, resulting in a lower relative effort and reducing the likelihood of breath-holding and straining," the statement reads.
The heart benefits of weight training include increased muscle mass which can help in weight control.
"Patients who have had cardiac events are often apprehensive about returning to this type of activity, or doing things in their daily lives that might be perceived as strenuous ... Now we know that they can return to the active things they enjoy doing," Williams said.
By recruiting new muscle fibers and increasing the body’s ability to use fuel, interval training could potentially lower the risk of metabolic syndrome.
Interval training does amount to hard work, but the sessions can be short. Best of all, a workout that combines tortoise and hare leaves little time for boredom.
Work Out Now, Ache Later: How Your Muscles Pay You Back
By Vicky Lowry : New York Times. November 16, 2004
Active people know the feeling all too well: a stiff and achy sensation in the muscles that sneaks up on the body 24 hours or more after, say, a hard run, a challenging weight lifting session or the first day back on the ski slopes.
Sports scientists call it delayed onset of muscle soreness. Athletes call it a nuisance because even simple movements like walking down stairs can be an ordeal. If the soreness is severe enough, it can hamper the next workout or even ruin a ski vacation.
Because of the delay, some people may not even realize that the aches and pains were caused by an activity - gardening, for example, or hammering nails - engaged in days before.
"I've had patients call me up who think they have a virus," said Dr. Gary Wadler, a professor at the New York University School of Medicine and a specialist in sports medicine.
The culprit for delayed muscle soreness is not, as some people used to think, the buildup of lactic acid, a byproduct of exercise that dissipates from the muscle tissues within an hour. That kind of soreness is considered acute. As soon as someone stops exercising, or shortly afterward, the burn goes away.
"It's not the key bad guy," said Dr. Michael Saunders, director of the Human Performance Laboratory at James Madison University in Harrisonburg, Va.
No one knows for sure exactly what does cause muscle soreness. But many scientists now think that the delayed pain is caused by microscopic tears in the muscles when a certain exercise or activity is new or novel. These tiny tears eventually produce inflammation, and corresponding pain, 24 to 36 hours later.
"White blood cells start to repair the damaged muscle after about 12 to 24 hours and they release a number of chemicals which are likely to be involved in the generation of local muscle pain," said Dr. Mark Tarnopolsky, a specialist in neuromuscular disorders at the McMaster University Medical Center in Hamilton, Ontario. "You see damage at the microscopic level immediately after exercise, yet the soreness is usually delayed for about 24 hours and peaks at 48 hours."
The good news is that as these little tears repair themselves, they prepare the muscles to handle the same type of exercise better the next time.
"The muscle gets more resilient, meaning the next time you do that same exercise you won't get damaged as much," said Dr. Priscilla Clarkson, a professor of exercise science at the University of Massachusetts and a leading researcher on muscle soreness. "That doesn't mean you are stronger, or mean you can lift more weight. It just means your muscle fibers are likely stronger so they won't tear as easily. Over time they'll build up and become a stronger fiber to lift more weight."
Performing certain exercises can almost guarantee delayed soreness: running, hiking or skiing downhill, for example, and lowering weights - what weight lifters refer to as "negatives." In these downhill or downward motions, called eccentric muscle actions, the muscle fibers have to lengthen and then contract, "like putting on the brakes," Dr. Clarkson explained. "It's that lengthening-contraction that puts the most strain on the fiber and does the most damage."
Of the 600 or so muscles in the human body, about 400 of them are skeletal. The largest of these are the muscles most susceptible to delayed soreness, Dr. Wadler said.
Severe muscle pain that lasts for many days can be a sign of rhabdomyolysis, a disorder that occurs when too much of the muscle protein myoglobin leaks from the muscle cells into the bloodstream, possibly damaging the kidneys.
Dark urine, indicating the presence of myoglobin, can be a symptom of rhabdomyolysis, which in very rare cases can lead to renal failure.
Running marathons and participating in other endurance events can cause rhabdomyolysis, said Dr. William O. Roberts, president of the American College of Sports Medicine. Other risk factors include being unfit or dehydrated and exercising in high temperatures.
"It's one of the reasons why you want to stay well hydrated if you are going to work your muscles hard," Dr. Roberts said. "Drink enough so that you have good urine output to clear these waste products." In most cases, though, delayed muscle soreness is not serious, and the soreness fades after a day or two of rest. Weight lifters typically work out the lower body one day and the upper body the next to give fatigued muscles a chance to recover. And conditioned athletes, like cyclists and runners, often alternate between easy and hard days of exercise. "Stress-adapt, stress-adapt so you can handle more and more exercise," said Dr. Tarnopolsky. "That's what an athlete strives for."
The results for other strategies for avoiding or recovering more quickly from muscle soreness are mixed. Many active people reach for nonsteroidal anti-inflammatory drugs like Advil or Aleve. While some data suggest that the drugs may work to prevent soreness or alleviate it once it sets in, the degree of reduction in soreness is small, Dr. Clarkson said.
Rarely, doctors prescribe the painkillers known as COX-2 inhibitors for short-term muscle soreness. But the drugs, which include Celebrex and Bextra, are more commonly used to treat arthritis.
And all cox-2 inhibitors are under increased scrutiny, after Vioxx was pulled from the market in September. Merck withdrew it after studies found it increased the risk of heart attacks and stroke.
Stretching does not prevent muscle soreness, researchers have found, and massage does little to improve recovery after eccentric muscle use, according to a study published in September in The American Journal of Sports Medicine. In the study, researchers in Stockholm found that after participants performed leg exercises to exhaustion, massage treatment did not affect the level or duration of pain, loss of strength or muscle function.
Consuming protein, however, may help. In a report published in the July issue of the journal Medicine & Science in Sports & Exercise, scientists found that trained cyclists who consumed a carbohydrate and protein beverage during and immediately after a ride, were able to ride 29 percent longer during the first ride, and 40 percent longer in a second session than those consuming carbohydrates alone.
"Our findings suggest that the protein-carbohydrate mix enhanced muscle performance and recovery in the later rides," said Dr. Saunders of James Madison, the study's lead author.
But further research is necessary. The results of the study may have been influenced by a higher caloric content in the carbohydrate-protein beverage.
"There is some evidence that consuming protein and carbohydrates in the immediate period after exercise may decrease subsequent muscle damage, but that research is in its infancy," said Dr. Tarnopolsky. "What has been fairly well established is that eating food in the postexercise period is better than starving.
"The take-home message is if you are training in the evening don't go to bed on an empty stomach. And if you work out in the morning, eat breakfast afterward or make darn sure to take a snack to work."
A practical tactic is to try to limit muscle soreness before it takes hold. For that, you need to train the body to get used to downhill or downward motions.
"Gradually run or walk down hills more if you are planning to participate in a downhill event, or take an elevator up to the top of a tall building and walk or run down the stairs," Dr. Roberts recommended.
Hikers should consider using adjustable poles, which distribute some of the stress on the legs, transferring it to the upper body, when descending steep grades. "I put hiking poles into the hands of every one of my clients and tell them that if they don't like them I'll carry them," said Nate Goldberg, who routinely guides hikes up 14,000-foot peaks in the Sawatch Mountains of Colorado as director of the Beaver Creek Hiking Center. "Very rarely do I get a set of poles back."
Seasoned athletes, it turns out, are no more immune to delayed onset of muscle soreness than neophyte exercisers. "If I asked Lance Armstrong to run down 10 flights of stairs, he'd be very sore," Dr. Clarkson said. "It's all about sport specificity."
Can Exercise Kill?
The answer: Yes, and probably more often than you think
By Kevin Helliker : Wall Street Journal : October 11, 2004
· In the space of seven months in 2002, three physicians at Johns Hopkins Hospital in Baltimore suffered sudden cardiac death while exercising. Two were running, the other working out in the hospital's fitness center. All three had paid close attention to diet and exercised regularly. The oldest was 51.
This unlikely string of deaths brought tremendous local attention to a topic that medicine typically doesn't emphasize -- for good reason. Exercise, after all, prolongs more lives than it cuts short. And in a nation that is largely sedentary, people need no extra excuse not to exercise.
Yet a growing number of physicians believe that publicizing the risks of exercise could potentially save a significant number of lives. Johns Hopkins cardiologist Nancy Strahan, for one, is now advising her middle-aged patients to stay away from jogging until they've undergone an exam to determine their risks.
"Present research reveals that vigorous exercise is responsible for triggering up to 17%" of sudden cardiac deaths in the U.S., says a recent article in the American Medical Athletic Association Journal. This means that vigorous exercise is triggering tens of thousands of U.S. deaths a year.
Impact on Immune System
What's more, sudden death isn't the only risk. Evidence is mounting that extreme exercise -- marathons, triathlons and the like -- may be detrimental to the immune system and long-term health. "Exercising to excess can harm our health," cautions Kenneth Cooper, the physician credited with founding the aerobics movement back in the 1960s.
All of this, of course, runs counter to conventional wisdom, which says that exercise is a virtue, and that you can't get too much of a virtue. Indeed, pretty much as soon as a thirtysomething slips on his first pair of running shoes he is challenged by an acquaintance or athletic-store poster to run a marathon. But exercise more accurately may be perceived as a medical therapy, and doctors are generally very cautious about the dosages they prescribe for medical therapies. Nobody would recommend quadrupling the dose of a drug that had proved to be effective.
So, how much is too much? It depends, of course, on the person.
The risk of sudden cardiac death during exercise would be reduced if people -- especially those older than 40 -- underwent various tests before starting a workout program. These tests include: an electrocardiogram, an electrical recording of the heart that can detect various abnormalities; an exercise stress test, during which physicians monitor the cardiovascular system's response during a treadmill workout; and an echocardiogram, an ultrasound scan that can spot a wide range of defects. Whether your insurance will pay for these tests depends on your age, health plan and how strongly your doctor recommends them.
Although these tests aren't guaranteed to find every cardiovascular booby trap that exercise can trip, they can identify a significant percentage of the conditions that cause sudden cardiac death-artery blockages, cardiac arrhythmias, aneurysms and more.
The risk of sudden death during exercise appears to rise as the duration of the workout grows. For instance, the risk of death during a marathon is about one in 50,000 finishers -- significantly higher than during shorter races or inactivity. One reason is that during long-distance runs the body sustains muscle injury, and it can react to this injury as if it were bleeding, by rendering blood more clottable, says Arthur Siegel, a Harvard University professor and chief of internal medicine at McLean Hospital in Belmont, Mass. In people with hidden blockage in their coronary arteries, this thickened blood can result in sudden cardiac death.
But that's not the only danger. Muscular injury can also set off a hormonal response that in turn triggers water intoxication, with acute brain swelling, says Dr. Siegel. This can be deadly for marathon runners who take too seriously the recommendation to drink lots of fluid. In recent years, young and healthy runners have died of hyponatremia -- essentially drinking too much fluid -- in several marathons, including those in Chicago and Boston.
"A half-million Americans a year are going out to run marathons," says Dr. Siegel. "They incur a dose of exercise that is enough to cause muscle injury that could, under certain circumstances, have grave consequences."
Having run 20 marathons himself, Dr. Siegel calls himself an advocate for safe participation. Avoiding hyponatremia is mostly a matter of drinking only when thirsty, and this caution is especially important for slower runners.
As for sudden cardiac death, Dr. Siegel suggests that people at risk for cardiac disease perhaps should be cautious about pushing their heart rates too high. People with high risk factors "ought to be careful about keeping the intensity moderate," says Dr. Siegel. "Exercise at a level where they can be conversational." Should such people run marathons? Dr. Siegel advises: "Do the marathon training but skip the race."
An increasingly popular theory has it that death from extreme exercise may not come until years afterward. This theory first occurred to Dr. Cooper, founder of the Cooper Institute in Dallas, when he noticed what seemed like a higher-than-average rate of cancer and other disease among the fitness fanatics he knew.
'More Harm Than Good'?
Having now studied the matter for more than 20 years, he has concluded that especially long and intense bouts of exercise may be damaging to the immune system. It is only a theory, but it is at least partly based on medical studies such as one showing that marathoners suffer a high rate of cold and flu just before and after races.
"If you're exercising more than five hours a week [at a high intensity], there's a possibility that you may be doing more harm than good," Dr. Cooper says.
Nobody should feel compelled for health reasons to run marathons, do triathlons or otherwise aspire to become a fitness fanatic, says Dr. Cooper, adding that 30 minutes a day of moderate exercise such as walking is sufficient.
Of course, there are benefits to extreme exercise -- it provides enormous relief from stress and consumes a spectacular number of calories. For people committed to exercising fanatically, Dr. Cooper and others recommend diets heavy in antioxidants such as green vegetables, as well as supplements such as vitamins C and E. Such diets are believed to bolster the immune system.
Devotees of extreme exercise express confidence that any risks, including a possible increased vulnerability to cancer, are outweighed by benefits ranging from lowered blood pressure to heightened confidence. This explains why Frank Webbe, a professor of psychology at Florida Institute of Technology, has run 14 marathons.
"You run them because you can," says Dr. Webbe, a veteran officer of a group called Running Psychologists. Marathons, he says, are "part of my identity. It's a self definition. I'm one of the elite few. It's important to me."
Is marathoning too good a thing for your heart?
By Gretchen Reynolds : NY Times article : December 7, 2006
HE had not expected to spend his 60th birthday in a hospital cardiac unit. R. J. Turner, a commercial real estate broker from Frederick County, Va., had planned a robust celebration. “I was going to finish my 10th marathon,” Mr. Turner said, “which isn’t bad for a guy my age.”
But near the start of the Marine Corps Marathon on Oct. 29, Mr. Turner raised an arm to wave at bystanders, and “everything went black.” Collapsing violently, he gashed his head, chipped a tooth and bit a deep hole in his bottom lip.
Mr. Turner, who had passed a stress test a year before, had just had a heart attack.
This has been an unusual season for the cardiac health of marathoners. After years in which almost no deaths were attributed to heart attacks at this country’s major marathons, at least six runners have died in 2006.
Two police officers, one 53, the other 60, died of heart attacks at the Los Angeles Marathon in March. The hearts of three runners in their early 40s gave out during marathons in Chicago in October, San Francisco in July and the Twin Cities in October. And at the same marathon where Mr. Turner was felled, another man, 56, crumpled near the 17th mile, never to recover.
This year’s toll has sobered race directors and medical directors of marathons. But, as Rick Nealis, the director of the Marine Corps Marathon, said, “Statistically, maybe, it was inevitable.”
Race fields have grown. In 2005, 382,000 people completed a marathon in the United States, an increase of more than 80,000 since 2000, according to marathonguide.com. Meanwhile, the risk of dying from a heart attack during a marathon is about 1 in 50,000 runners, said Dr. Arthur Siegel, the director of internal medicine at McLean Hospital in Belmont, Mass., and an assistant professor of medicine at Harvard.
But some physicians, including Dr. Siegel, an author of more than two dozen studies of racers at the Boston Marathon, wonder if there is more to the deaths than mathematical inevitability: Does racing 26.2 miles put a heart at risk?
A new study by Dr. Siegel and colleagues at Massachusetts General Hospital and other institutions is at least suggestive. Sixty entrants from the 2004 and 2005 Boston Marathon were tested before and after the race. Each was given an echocardiogram to find abnormalities in heart rhythm and was checked for blood markers of cardiac problems — in particular for troponin, a protein found in cardiac muscle cells. If the heart is traumatized, troponin can show up in the blood. Its presence can determine whether there has been damage from a heart attack.
The runners (41 men, 19 women) had normal cardiac function before the marathon, with no signs of troponin in their blood. Twenty minutes after finishing, 60 percent of the group had elevated troponin levels, and 40 percent had levels high enough to indicate the destruction of heart muscle cells. Most also had noticeable changes in heart rhythms. Those who had run less than 35 miles a week leading up to the race had the highest troponin levels and the most pronounced changes in heart rhythm.
The findings, published in the Nov. 28 issue of Circulation, a journal of the American Heart Association, were a surprise, and not least to the runners. None had reported chest pains or shortness of breath at the finish. All had felt fine, Dr. Siegel said (to the extent one can feel fine after pounding through 26.2 miles).
Within days, the abnormalities disappeared. But something seemed to have happened in the race. “Their hearts appeared to have been stunned,” Dr. Siegel said.
“Although the evidence is not conclusive, it does look like the Boston study is showing some effect on cardiac muscle,” said Dr. Paul D. Thompson, 59, the director of cardiology at Hartford Hospital in Connecticut, and an author of an editorial that accompanied the study. “It’s far too early to draw any conclusions,” he added. “We’d be seeing lots more bodies piling up if there were real lingering long-term cardiac damage” caused by running marathons.
“Over all, the evidence is strongly in favor of the idea that endurance exercise is helpful in terms of cardiac health,” said Dr. Thompson, who has run more than 30 marathons.
But questions do remain. Another new study, this one out of the University of Duisburg-Essen in Germany, showed completely unexpected results in a group of experienced middle-aged male marathoners. In the study, which was presented in November at a meeting of the American Heart Association, the subjects, each of whom had completed at least five marathons, underwent an advanced type of heart screening called a spiral CT scan. Unlike echocardiograms or stress tests, spiral CTs show the level of calcium plaque buildup or atherosclerosis in the arteries.
More than a third of the runners had significant calcium deposits, suggesting they were at relatively high risk for a heart attack. Only 22 percent of a control group of nonrunners had a comparable buildup.
The researchers scrupulously avoided suggesting that marathoning had caused the men to develop heart disease. (After all, running may have kept them alive when they would otherwise have keeled over years earlier.) But neither did the authors rule out the possibility that in some baffling way distance running had contributed to the men’s arterial gunk.
What worries Dr. Siegel and some of his colleagues is that marathons present an opportunity for silent symptomless heart disease to introduce itself abruptly. The pulsing excitement, the adrenaline, the unpleasant process of “hitting the wall” may trigger physiological changes that loosen arterial plaques, precipitating a heart attack, Dr. Siegel said.
His advice to runners with any history of heart trouble is “train for the race, getting the cardiac benefits of endurance exercise,” then watch the event on television.
The risk of going into cardiac arrest as a spectator, he said, is only about one in a million. (The applicable studies of spectators involved Super Bowl fans.)
Anyone considering joining the ranks of marathoners should undergo a full medical screening, with a visit to a cardiologist for those over 40, Dr. Siegel said. Spiral CT scans are desirable (the cost can range from $250 to $850) and are covered by insurance if recommended by a physician.
Those with a family history of cardiac problems should be especially cautious. “You can’t outrun your genes,” Dr. Siegel said, a reality that marathon medical experts call the Jim Fixx effect, after the author of “The Complete Book of Running,” who died of a heart attack in 1984 at 52. His father had also died young.
Still, the majority of cardiologists remain avid fans of marathons. “It is an extraordinary event,” said Dr. Frederick C. Lough, the director of cardiac surgery at George Washington University in Washington. “But you have to respect that distance. It’s not something everyone necessarily should attempt.”
Dr. Lough, 57, was less than a block behind Mr. Turner when the older man collapsed. He interrupted his own race to help revive Mr. Turner and accompany him to the hospital, before completing the marathon. “It was a vivid reminder that running does not make anyone immune to heart disease,” Dr. Lough said.
Experts familiar with the new cardiac studies of marathoners urge caution and perspective. The numbers of people studied were small, the findings unexplained, and results have not yet been replicated.
Don’t use the studies, in other words, to justify parking yourself smugly on the couch. “There’s not yet in my opinion cause for alarm,” Dr. Thompson said. “I would still tell people, run.”
His words doubtless will cheer Mr. Turner. “You know the worst thing about almost dying?” he said. “That I didn’t finish.” After having had a stent installed in his heart to open an artery that was about 98 percent blocked, he’s now walking a mile a day and planning his comeback. “I want to get that 10th marathon in,” he said.
But not before he gets a full medical screening, including a spiral CT scan.
·
Fitness: It’s O.K. to Run Hurt
By Gina Kolata ; NY Times article : January 11, 2007
JUST before the end of last year, a prominent orthopedic surgeon was stretching to lift a heavy box and twisted his back. The pain was agonizing. He could not sit, and when he lay down he could barely get up.
So the surgeon, Dr. James Weinstein of Dartmouth College, decided to go out for a run.
“I took an anti-inflammatory, iced up, and off I went,” Dr. Weinstein recalled. When he returned, he said, he felt “pretty good.”
It sounds almost like heresy. The usual advice in treating injuries is to rest until the pain goes away. But Dr. Weinstein and a number of leading sports medicine specialists say that is outdated and counterproductive. In fact, Dr. Weinstein says, when active people consult him, he usually tells them to keep exercising.
The idea, these orthopedists and exercise specialists say, is to use common sense. If you’ve got tendinitis or sprained a muscle or tendon by doing too much, don’t go right back to exercising at the same level.
The specific advice can differ from specialist to specialist. Some, like Dr. Weinstein, say most people can continue with the sport they love although they may need to cut back a bit, running shorter distances or going more slowly. Others say to cross-train at least some of the time and others say the safest thing to do is to cross-train all the time until the pain is gone. You might end up cycling instead of running, or swimming instead of playing tennis. But unless it’s something as serious as a broken bone or a ripped ligament or muscle, stopping altogether may be the worst thing to do.
“We want to keep you moving,” said Dr. William Roberts, a sports medicine specialist at the University of Minnesota and a past president of the American College of Sports Medicine. “Injured tissue heals better if it’s under some sort of stress.”
He and others acknowledge that the advice to keep moving may come as a surprise and that some doctors feel uncomfortable giving it, worried that their patients will do too much, make things worse and then blame their doctor.
“I’m not convinced this is part of every doctor’s training or that everyone is ready to make it part of mainstream medicine,” Dr. Roberts said. “You have to work with athletes a while to figure out how to do it and how to do it well.”
“The easy way out is to say, ‘Don’t exercise,’ ” said Dr. Richard Steadman, an orthopedic surgeon in Vail, Colo., and founder of the Steadman Hawkins Research Foundation, which studies the origins and treatment of sports injuries. That advice, he added, “is safe and you probably will have healing over time.” But, he said, “if the injury is not severe, resting it will probably prolong recovery.”
Medical researchers say that they only gradually realized the importance of exercising when injured. A few decades ago, Dr. Mininder Kocher, a sports medicine specialist and orthopedic surgeon at Children’s Hospital Boston, said doctors were so intent on forcing hurt athletes to rest that they would put injured knees or elbows or limbs in a cast for two to three months.
When the cast finally came off, the patient’s limb would be stiff, the muscles atrophied. “It would take six months of therapy to get strength and motion back,” Dr. Kocher said.
At the same time, in a parallel path, researchers were learning that painful conditions that are essentially inflammation — arthritis and chronic lower back pain — actually improve when patients keep moving.
Now some researchers, like Dr. Freddie Fu, a sports medicine expert and chairman of the orthopedic surgery department at the University of Pittsburgh Medical Center, and a colleague, James H-C. Wang, are studying minor injuries at the molecular level.
Their focus is on tendinitis — the inflamed tendons that are the bane of many exercisers and that affect 15 to 20 percent of all Americans at any given time. The symptoms are all too familiar — pain, swelling and soreness. To study the injury process, Dr. Wang grows human tendons in the laboratory, stretching them repeatedly. In separate experiments, he has mice run on treadmills until their tendons begin to show the tiny microscopic tears that occur in the early stages of tendinitis.
So far, Dr. Wang reports, he and Dr. Fu learned some important lessons: First, forceful stretching of tendons elicits the production of molecules that are involved in inflammation. But small repeated stretching of tendons that are already inflamed leads to the production of molecules that heal inflammation. That suggests moderate exercise can actually speed healing.
And now, their preliminary results suggest that the usual treatment for tendinitis — taking drugs like aspirin or ibuprofen — can help reduce inflammation when the injury begins. But after inflammation is under way, they can make matters worse.
But medical experts caution that people have to be careful if they try to exercise when they are injured.
Some, like Dr. Fu, who is himself a cyclist, Dr. Roberts, and Dr. Steadman say the first priority is to see a doctor and get an accurate diagnosis in order to rule out a serious injury.
Others, like Dr. Weinstein, say that such an injury, a broken bone or a torn Achilles tendon, for example, has symptoms so severe that it is obvious something is really wrong.
“If you had inflammation and swelling that was very tender to the touch, you would know,” Dr. Weinstein said. And if you tried to exercise, it would hurt so much that you just could not do it.
Dr. Weinstein’s advice for injured patients is among the boldest — he said it’s based on his basic research and his own experience with sports injuries, like knee pain and tendinitis of the Achilles and hamstring. Before exercise, he said, take one anti-inflammatory pill, like an aspirin. Ice the area for 20 minutes. Then start your usual exercise, the one that resulted in your injury, possibly reducing the intensity or time you would have spent. When you finish, ice the injured area again.
The advice involving an anti-inflammatory pill, Dr. Weinstein said, is based on something surgeons know — in most cases, a single anti-inflammatory pill before surgery results in less pain and swelling afterward. It also is consistent with Dr. Wang’s research because, at least in theory, it should forestall new inflammation from the exercise that is about to occur.
The icing is to constrict blood vessels before and after exercise, thereby preventing some of the inflammatory white blood cells from reaching the injured tissue.
Dr. Steadman, who works with injured athletes in his clinic, does not advise trying to go back to your old exercise on your own until the pain is completely gone. Play it safe, he said, and cross-train.
But others, like Dr. Fu and Dr. Kocher, are more inclined to suggest trying your old sport. Both also tell injured patients to ice before and after exercising. Dr. Kocher said he sometimes advises taking an anti-inflammatory pill, but worries about masking pain so much that patients injure themselves even more by overdoing the exercise.
His rule of thumb, Dr. Kocher said, is that if the pain is no worse after exercising than it is when the person simply walks, then the exercise “makes a lot of sense.”
It also helps patients psychologically, he added. “If you take athletes or active people out, they get depressed, they get wacky,” Dr. Kocher explained.
Noah Hano knows all about that.
Mr. Hano, 34, a commercial real estate broker in Boston, was competing in marathons and triathlons. Then he developed severe sciatica, whose pain is a direct result of inflammation. He tried physical therapy, he tried acupuncture, he tried massage therapy, but nothing quelled the “nagging, terrible pain” down his leg, he said.
He stopped exercising, but the pain persisted.
“I started getting desperate,” Mr. Hano said. His father, who lives in the same town as Dr. Weinstein, suggested that Mr. Hano call the Dartmouth orthopedist. Dr. Weinstein told him to continue to exercise. Mr. Hano could not wait to get started. “I drove to the gym and ran on the treadmill,” he said. “When I woke up the next morning, I went for a swim and rode my bike. It hurt, but when the doctor told me I wasn’t going to be paralyzed, it made it a lot easier.”
Dr. Weinstein said that Mr. Hano’s problem was a huge, bulging disk, a herniation so severe that most doctors would say he should stop running immediately. Dr. Weinstein, though, thought exercise would help Mr. Hano heal. His treatment was a single injection of cortisone into the inflamed area around his disk. The sciatica gradually went away. And Mr. Hano continues to run.
“I had faith that I was going to be able to work through it,” Mr. Hano said. “I don’t want to not do what I like just because I’m in pain.”
Daily supplements
By Gretchen Reynolds : NY Times article : March 4, 2007
It’s no surprise that athletes like their dietary supplements. By conservative estimates, they spend nearly $4 billion annually on pills, powders and other sports-nutrition products in the hope that they’ll improve health and increase performance. New Orleans Saints center Jeff Faine recently told a reporter that he takes about 65 pills a day; for the sake of time management, he has taught himself to swallow as many as 17 at a time. This daily gorging pales next to that of Bill Romanowski, the former linebacker. In his 2005 autobiography, “Romo: My Life on the Edge,” Romanowski writes that he kept a tackle box filled with some 500 pills and would take handfuls a day, all washed down with protein shakes. He also famously admits to taking vials of THG, an anabolic steroid, but most of what he consumed were legal supplements available at any Walgreens or GNC store.
· Such supplements are not necessarily benign. In 2003, Baltimore Orioles pitcher Steve Bechler died, in part, from a reaction to ephedrine, a wildly popular supplement used to increase energy and metabolism. Ephedrine, a stimulant derived from the ephedra plant, can elevate heart rate and blood pressure, in some cases fatally. It’s now illegal to market ephedrine as a dietary supplement, though it’s still widely available, often as a decongestant or a cold remedy. Sales are brisk.
· Which underscores the disturbing truth about supplements: science and common sense often have less effect on their use than hope, hype and word of mouth. “A lot of the information about supplements is generated by the manufacturers or by personal testimonials,” says Kathleen Laquale, a leading nutritionist and an associate professor of athletic training at Bridgewater State College in Massachusetts. “Someone at the machine next to you in the gym says, ‘You’ve got to try this.’ ”
· That person could be right. Some supplements do what they promise. But the vast majority are ineffective — hard news for people (like me) who load up on vitamins and other pills and powders in the belief that they must be doing something. So how to separate the dross from the goods? Aside from the obvious — don’t take a supplement you haven’t thoroughly researched — it’s a matter of trial and error. What works for others might not work for you. Also bear in mind that positive results may have more to do with what’s going on in your mind than in your body. Try a high-profile supplement, some of the most popular of which are discussed here, and chances are you’ll swear it works, even if, strictly speaking, it doesn’t. The placebo effect, Laquale says, “is still an effect.”
Vitamins and Minerals: Way Too Much of a Good Thing
Unless you’re on an outré diet (grapefruit, cabbage soup, even Atkins), you’re probably getting enough daily nutrients without help from pills. “Most Americans easily get 100 percent of the vitamins and minerals they need from their food,” says Ellen Coleman, a sports dietician who consults for the Los Angeles Lakers and Angels.
It’s often presumed, however, that athletes need more than their three balanced meals a day. Heavy exertion increases the body’s use of oxygen and subsequently produces more free radicals: unstable atoms and molecules known to be harmful to cells. In theory, athletes should benefit from extra doses of antioxidants like vitamins C and E, beta carotene and coenzyme Q10, which reduce free radicals.
But research has produced mixed results. Several recent studies of animals suggested that large single doses of antioxidants (1,000 I.U. of vitamin E, say, instead of 100 I.U.) actually increased signs of oxidative damage; other studies have suggested that antioxidants might help speed muscle recovery, particularly for older athletes. To further the confusion, researchers have recently speculated that those who exercise less vigorously could possibly benefit more from antioxidant supplements than could elite athletes, whose bodies, the thinking now goes, might be better equipped to combat oxidative stress.
Athletes also tend to overdo the B-complex vitamins. Because B vitamins are essential for turning carbohydrates, fats and proteins into energy, many vitamins contain — and trumpet on their labels — mega-doses of the stuff. But “there’s not much evidence that extra doses of B vitamins give you better athletic performance or anything else,” Laquale says — besides a lighter wallet.
If you still can’t bear the thought of parting with your vitamins, limit yourself to a one-a-day multivitamin. “It’s hard to overdose on any one nutrient that way,” says Alicia Kendig, a sports dietician with Carmichael Training Systems in Colorado Springs, “and it gives you that little bit of extra insurance that you’re getting all the nutrients you need.”
Creatine: Speed, Strength and Some Minor Gastric Upset
Creatine, an amino acid compound stored in muscle tissue, is the top-selling sports supplement in the country. Available in powdered form, it aids the production of phosphocreatine (PCr), an important fuel used during short, intense exercise.
This is one supplement that actually seems to work. “There’s solid research that creatine helps to increase muscle mass and strength,” Coleman says. One recent study of male United S tates Army soldiers found that those taking creatine could do 14 percent more bench press repetitions than those taking a placebo. And a 2002 study conducted by Australian researchers showed that elite female soccer players who took the supplement were faster in a series of sprints than those on a placebo.
But creatine’s benefits are limited to activities that demand strength or short bursts of speed. It won’t do much for marathoners or other distance athletes. It’s not gentle on the system, either. Creatine pulls water into muscles, and in the process can dehydrate the rest of the body. Studies done in the late 1990s suggested that there were links between the supplement and muscle cramping and diarrhea, but those side effects were found at doses higher than what is generally recommended today. Coleman says five grams a day should get you the benefits without too much . . . distress.
DHEA: Increased Productivity at the Testosterone Factory?
Dehydroepiandrosterone, or DHEA, is a hormone produced naturally in human adrenal glands. Without it, the body can’t make testosterone or estrogen. Because of this link to testosterone, many athletes take DHEA capsules in the hope of building more muscle.
Studies conducted in the 1990s showed that rats and mice developed stronger bones, muscles and immune systems when given DHEA. Rodents, however, produce little DHEA naturally, so some researchers speculated that the supplement merely acted as a temporary jolt to their systems. Although a few small studies suggested that some elderly people with low levels of DHEA benefited from taking the supplements, the overall results were equivocal.
Then last October, in the , New England Journal of Medicine researchers from the Mayo Clinic published the results of a two-year, double-blind study on the efficacy of DHEA. The study found no beneficial effects. A 75-milligram daily dose for men did increase blood levels of DHEA but didn’t increase muscle strength or oxygen consumption. Neither did it decrease body fat. DHEA had no “physiologically relevant beneficial effects,” the authors concluded.
Undeterred, the Council for Responsible Nutrition, a trade group for the supplement industry, released a statement saying that the Mayo study confirmed “the safety of relatively high-dose DHEA.” It didn’t work, but it didn’t kill anyone, either.
It’s this kind of cheery obfuscation that keeps the supplement industry humming. “The amount of deliberate misinformation out there is amazing,” Laquale says. “It would be funny if it weren’t so disturbing.”
Because the Food and Drug Administration doesn’t closely regulate the nutritional supplement business — a 1994 law exempted supplements from strict oversight — the claims made by manufacturers tend to be extravagant. (“Instantly Triggers Extreme Muscle Expansion!”) The fine print adds that these statements have not been evaluated by the F.D.A. “But most people don’t read that far,” Coleman says.
Where, then, can you look for reliable, unbiased information? One place to start is ConsumerLab.com, an independent research organization that tests supplements. A yearly subscription to the site, which posts all of the lab’s product reports, costs $27.
In some instances, supplements tested by ConsumerLab have been found to contain ingredients not printed on their labels. A recent test of weight-loss supplements found that some were contaminated with lead. More often, though, the lab discovers what’s not in the supplement. ConsumerLab’s creatine study, for example, revealed products that contained little or no creatine at all. “The labels of supplements can be misleading,” says Tod Cooperman, a medical doctor who specializes in pharmaceuticals and is ConsumerLab’s president. “You should always be skeptical.”
One abiding fact about supplements is that their allure waxes and ebbs. The newest “it” supplement is resveratrol, a substance found in the skin of red grapes that was recently shown to protect against weight gain in rodents and to almost double the animals’ endurance on a treadmill. Since the results of this research were announced last year, companies have been scrambling to produce resveratrol formulations. Dozens are now available.
Studies have yet to be conducted to determine whether resveratrol improves performance in humans. Until then, it might be easier just to swallow your vitamins with a glass of Shiraz.
Exercise Overview
Physical activity is any activity that causes your body to work harder than normal. The actual amount of physical activity you need depends on your fitness goals, whether you are trying to lose weight, and how fit you are right now.
Physical activity can help you:
The number of calories burned during physical activity depends on:
Your basal metabolic rate (BMR) is the number of calories your body uses when it is at rest. BMR accounts for most of your calorie use. Your basal metabolic rate is based on things your body always does such as breathing, breaking down food, and keeping your heart and brain working. Your age, sex, body weight, and level of physical activity affect the basal metabolic rate. Basal metabolic rate increases with the amount of muscle tissue you have, and it reduces with age.
Along with burning more calories, physical activity increases the BMR, and the BMR can remain increased after 30 minutes of moderate physical activity. For many people, the basal metabolic rate can be increased for approximately 48 hours after the activity. This means, for example, that after the physical activity, when a person is sitting and watching television, the body is using more calories than usual.
EFFECT ON APPETITE
Physical activity at a moderate rate does not increase the appetite. In some situations, the appetite will actually decrease. Research shows that the decrease in appetite after physical activity is greater in individuals who are obese than in individuals who are at their right body weight.
LOSS OF BODY FAT
When losing weight just by taking in less calories, a person loses a quarter of his or her lean body mass, and three quarters of his or her body fat. Combining calorie reduction with physical activity can result in loss of 98% of body fat. Weight loss that is reached with a combination of calorie reduction and physical activity is more effective. For keeping a desirable body weight, a maintenance level of calories along with physical activity is recommended. This helps to preserve lean body mass and muscle tone.
RECOMMENDATIONS
For losing or maintaining weight:
Physical activity at 60 to 70% of the maximum heart rate can be continued safely for a long period of time. If an exercise is too hard, conversation cannot be carried on during the physical activity (the person is out of breath).
According to the American College of Sports Medicine, physical activity of less than 2 times a week at less than 60% of the maximum heart rate, and for less than 10 minutes per day, does not help in developing and maintaining fitness. If physical activity is stopped, the fitness benefits are completely lost. Within 2 to 3 weeks the level of fitness is reduced, and within 3 to 8 months it is completely lost, and the person has to restart again.
Twenty minutes of continuous aerobic activity 3 days per week is recommended for weight loss. Examples of physical activity that are considered aerobic are: walking, running, jogging, hiking, swimming, bike riding, rowing, cross country skiing, and jumping rope.
BENEFITS
Physical activity contributes to health by reducing the heart rate, decreasing the risk for cardiovascular disease, and reducing the amount of bone loss that is associated with age and osteoporosis. Physical activity also helps the body use calories better, thereby helping with weight loss and weight maintenance. It can increase basal metabolic rate, reduces appetite, and help in the reduction of body fat.
SIDE EFFECTS
Physical activity should be done at a rate that is right for the person. An evaluation by an exercise physiologist is helpful, in order to to avoid injuries. Injuries can occur if physical activity is started without much consideration as to the type or length of the activity, and the physical condition of the person.
Does Exercise Really Keep Us Healthy?
By Gina Kolata : NY Times Article : January 8, 2008
Exercise has long been touted as the panacea for everything that ails you. For better health, simply walk for 20 or 30 minutes a day, boosters say — and you don’t even have to do it all at once. Count a few minutes here and a few there, and just add them up. Or wear a pedometer and keep track of your steps. However you manage it, you will lose weight, get your blood pressure under control and reduce your risk of osteoporosis.
If only it were so simple. While exercise has undeniable benefits, many, if not most, of its powers have been oversold. Sure, it can be fun. It can make you feel energized. And it may lift your mood. But before you turn to a fitness program as the solution to your particular health or weight concern, consider what science has found.
Moderate exercise, such as walking, can reduce the risk of diabetes in obese and sedentary people whose blood sugar is starting to rise. That outcome was shown in a large federal study in which participants were randomly assigned either to an exercise and diet program, to take a diabetes drug or to serve as controls. Despite trying hard, those who dieted and worked out lost very little weight. But they did manage to maintain a regular walking program, and fewer of them went on to develop diabetes.
Exercise also may reduce the risk of heart disease, though the evidence is surprisingly mixed. There seems to be a threshold effect: Most of the heart protection appears to be realized by people who go from being sedentary to being moderately active, usually by walking regularly. More intense exercise has been shown to provide only slightly greater benefits. Yet the data from several large studies have not always been clear, because those who exercise tend to be very different from those who do not.
Active people are much less likely to smoke; they’re thinner and they eat differently than their sedentary peers. They also tend to be more educated, and education is one of the strongest predictors of good health in general and a longer life. As a result, it is impossible to know with confidence whether exercise prevents heart disease or whether people who are less likely to get heart disease are also more likely to be exercising.
Scientists have much the same problem evaluating exercise and cancer. The same sort of studies that were done for heart disease find that people who exercised had lower rates of colon and breast cancer. But whether that result is cause or effect is not well established.
Exercise is often said to stave off osteoporosis. Yet even weight-bearing activities like walking, running or lifting weights has not been shown to have that effect. Still, in rigorous studies in which elderly people were randomly assigned either to exercise or maintain their normal routine, the exercisers were less likely to fall, perhaps because they got stronger or developed better balance. Since falls can lead to fractures in people with osteoporosis, exercise may prevent broken bones — but only indirectly.
And what about weight loss? Lifting weights builds muscles but will not make you burn more calories. The muscle you gain is minuscule compared with the total amount of skeletal muscle in the body. And muscle has a very low metabolic rate when it’s at rest. (You can’t flex your biceps all the time.)
Jack Wilmore, an exercise physiologist at Texas A & M University, calculated that the average amount of muscle that men gained after a serious 12-week weight-lifting program was 2 kilograms, or 4.4 pounds. That added muscle would increase the metabolic rate by only 24 calories a day.
Exercise alone, in the absence of weight loss, has not been shown to reduce blood pressure. Nor does it make much difference in cholesterol levels. Weight loss can lower blood pressure and cholesterol levels, but if you want to lose weight, you have to diet as well as exercise. Exercise alone has not been shown to bring sustained weight loss.Just ask Steven Blair, an exercise researcher at the University of South Carolina. He runs every day and even runs marathons. But, he adds, “I was short, fat and bald when I started running, and I’m still short, fat and bald. Weight control is difficult for me. I fight the losing battle.”
The difficulty, Dr. Blair says, is that it’s much easier to eat 1,000 calories than to burn off 1,000 calories with exercise. As he relates, “An old football coach used to say, ‘I have all my assistants running five miles a day, but they eat 10 miles a day.’”
Preserving a Fundamental Sense: Balance
By Jane E. Brody : NY Times Article : January 8, 2008
Scott McCredie is a Seattle-based health and science writer who says he “discovered” what he calls “the lost sense” of balance after he watched in horror as his 67-year-old father tumbled off a boulder and disappeared from sight during a hike in the Cascades.
Though his father hurt little more than his pride, Mr. McCredie became intrigued by what might have caused this experienced hiker, an athletic and graceful man, to lose his balance suddenly. His resulting science-and-history-based exploration led to a book, “Balance: In Search of the Lost Sense,” published last June by Little, Brown.
Noting that each year one in three Americans 65 and older falls, and that falls and their sometimes disastrous medical consequences are becoming more common as the population ages, Mr. McCredie wonders why balance is not talked about in fitness circles as often as strength training, aerobics and stretching. He learned that the sense of balance begins to degrade in one’s 20s and that it is downhill — literally and figuratively — from there unless steps are taken to preserve or restore this delicate and critically important ability to maintain equilibrium.
Vertigo, which can be caused by inner ear infections, low blood pressure, brain injuries, certain medications and some chronic diseases, is loss of balance in the extreme. Anyone who has experienced it — even if just from twirling in a circle — knows how disorienting and dangerous it can be. Really, without a sense of balance, just about everything else in life can become an insurmountable obstacle.
One normal consequence of aging is a steady decline in the three main sensory contributors to good balance — vision, proprioceptors on the bottoms of the feet that communicate position information to the brain, and the tiny hairs in the semicircular canals of the inner ear that relay gravity and motion information to the brain. Add to that the loss of muscle strength and flexibility that typically accompany aging and you have a fall waiting to happen.
But while certain declines with age are unavoidable, physical therapists, physiatrists and fitness experts have repeatedly proved that much of the sense of balance can be preserved and even restored through exercises that require no special equipment or training. These exercises are as simple as standing on one foot while brushing your teeth or walking heel-to-toe with one foot directly in front of the other.
Testing for Equilibrium
Marilyn Moffat and Carole B. Lewis, physical therapists in New York and Washington, respectively, agree with Mr. McCredie that “balance is an area of physical fitness that is often overlooked,” but they seek to correct that in their recent book “Age-Defying Fitness” (Peachtree Publishers). They define balance as “the ability of your body to maintain equilibrium when you stand, walk or perform any other daily activity” like putting on pants, walking on uneven ground or reaching for something on a shelf.
Dr. Moffat and Dr. Lewis suggest starting with a simple assessment of your current ability to maintain good balance. With a counter or sturdy furniture near enough to steady you if needed, perform this test:
1. Stand straight, wearing flat, closed shoes, with your arms folded across your chest. Raise one leg, bending the knee about 45 degrees, start a stopwatch and close your eyes.
2. Remain on one leg, stopping the watch immediately if you uncross your arms, tilt sideways more than 45 degrees, move the leg you are standing on or touch the raised leg to the floor.
3. Repeat this test with the other leg.
Now, compare your performance to the norms for various ages:
¶ 20 to 49 years old: 24 to 28 seconds.
¶ 50 to 59 years: 21 seconds.
¶ 60 to 69 years: 10 seconds.
¶ 70 to 79 years: 4 seconds.
¶ 80 and older: most cannot do it at all.
If you are wise, whatever your age, you will want to strive for the norm of those younger than 50. To increase stability and strengthen the legs, stand with feet shoulder-width apart and arms straight out in front. Lift one foot behind, bending the knee at 45 degrees. Hold that position for five seconds or longer, if possible.
Repeat this exercise five times. Then switch legs. As you improve, try one-leg stands with your eyes closed.
You can also incorporate one-leg stands into daily routines — while on the telephone, for example, brushing your teeth, waiting in line or for a bus, or cooking and washing dishes.
Exercises to Build a Motor Skill
“Remember, balance is a motor skill,” Dr. Moffat, professor of physical therapy at New York University, said in an interview. “To enhance it, you have to train your balance in the same way you would have to train your muscles for strength and your heart for aerobic capacity.”
Dr. Moffat pointed out that balance is twofold: static while standing still and dynamic when moving, as in walking and climbing stairs. Two main routes improve balance — exercises that increase the strength of the ankle, knee and hip muscles and exercises that improve the function of the vestibular system.
Like one-leg stands, many can be done as part of a daily routine. Dr. Moffat recommends starting with strength exercises and, as you improve, adding vestibular training by doing some of them with closed eyes.
Sit-to-stand exercises once or twice a day increase ankle, leg and hip strength and help the body adjust to changes in position without becoming dizzy after being sedentary for a long time. Sit straight in a firm chair (do not lean against the back) with arms crossed. Stand up straight and sit down again as quickly as you can without using your arms. Repeat the exercise three times and build to 10 repetitions.
Heel-to-toe tandem walking is another anytime exercise, resembling plank walking popular with young children. It is best done on a firm, uncarpeted floor. With stomach muscles tight and chin tucked in, place one foot in front of the other such that the heel of the front foot nearly touches the toe of the back foot. Walk 10 or more feet and repeat the exercise once or twice a day.
Also try walking on your toes and then walking on your heels to strengthen your ankles.
Another helpful exercise is sidestepping. Facing a wall, step sideways with one leg (bring the other foot to it) 10 times in each direction. After mastering that, try a dancelike maneuver that starts with sidestepping once to the right. Then cross the left leg behind, sidestep to the right again and cross the left leg in front. Repeat this 10 times. Then do it in the other direction.
In addition, the slow, continuous movements of tai chi, that popular Chinese exercise, have been shown in scientific studies to improve balance and reduce the risk of falls.
The Simple Push-Up as a sign of health and wellness
By Tara Parker-Pope : NY Times Article : March 11, 2008
As a symbol of health and wellness, nothing surpasses the simple push-up.
Practically everyone remembers the actor Jack Palance performing age-defying push-ups during his Oscar acceptance speech. More recently, Randy Pausch, the Carnegie Mellon professor whose last lecture became an Internet sensation, did push-ups to prove his fitness despite having pancreatic cancer.
"It takes strength to do them, and it takes endurance to do a lot of them," said Jack LaLanne, 93, the fitness pioneer who astounded television viewers in the 1950s with his fingertip push-ups. "It's a good indication of what kind of physical condition you're in."
The push-up is the ultimate barometer of fitness. It tests the whole body, engaging muscle groups in the arms, chest, abdomen, hips and legs. It requires the body to be taut like a plank with toes and palms on the floor. The act of lifting and lowering one's entire weight is taxing even for the very fit.
"You are just using your own body and your body's weight," said Steven G. Estes, a physical education professor and dean of the college of professional studies at Missouri Western State University. "If you're going to demonstrate any kind of physical strength and power, that's the easiest, simplest, fastest way to do it."
But many people simply can't do push-ups. Health and fitness experts, including the American College of Sports Medicine, have urged more focus on upper-body fitness. The aerobics movement has emphasized cardiovascular fitness but has also shifted attention from strength training exercises.
Moreover, as the nation gains weight, arms are buckling under the extra load of our own bodies. And as budgets shrink, public schools often do not offer physical education classes — and the calisthenics that were once a childhood staple.
In a 2001 study, researchers at East Carolina University administered push-up tests to about 70 students ages 10 to 13. Almost half the boys and three-quarters of the girls didn't pass.
Push-ups are important for older people, too. The ability to do them more than once and with proper form is an important indicator of the capacity to withstand the rigors of aging.
Researchers who study the biomechanics of aging, for instance, note that push-ups can provide the strength and muscle memory to reach out and break a fall. When people fall forward, they typically reach out to catch themselves, ending in a move that mimics the push-up. The hands hit the ground, the wrists and arms absorb much of the impact, and the elbows bend slightly to reduce the force.
In studies of falling, researchers have shown that the wrist alone is subjected to an impact force equal to about one body weight, says James Ashton-Miller, director of the biomechanics research laboratory at the University of Michigan.
"What so many people really need to do is develop enough strength so they can break a fall safely without hitting their head on the ground," Dr. Ashton-Miller said. "If you can't do a single push-up, it's going to be difficult to resist that kind of loading on your wrists in a fall."
And people who can't do a push-up may not be able to help themselves up if they do fall.
"To get up, you've got to have upper-body strength," said Peter M. McGinnis, professor of kinesiology at State University of New York College at Cortland who consults on pole-vaulting biomechanics for U.S.A. Track and Field, the national governing body for track.
Natural aging causes nerves to die off and muscles to weaken. People lose as much as 30 percent of their strength between 20 and 70. But regular exercise enlarges muscle fibers and can stave off the decline by increasing the strength of the muscle you have left.
Women are at a particular disadvantage because they start off with about 20 percent less muscle than men. Many women bend their knees to lower the amount of weight they must support. And while anybody can do a push-up, the exercise has typically been part of the male fitness culture. "It's sort of a gender-specific symbol of vitality," said R. Scott Kretchmar, a professor of exercise and sports science at Penn State. "I don't see women saying: 'I'm in good health. Watch me drop down and do some push-ups.' "
Based on national averages, a 40-year-old woman should be able to do 16 push-ups and a man the same age should be able to do 27. By the age of 60, those numbers drop to 17 for men and 6 for women. Those numbers are just slightly less than what is required of Army soldiers who are subjected to regular push-up tests.
If the floor-based push-up is too difficult, start by leaning against a countertop at a 45-degree angle and pressing up and down. Eventually move to stairs and then the floor.
Mr. LaLanne, who once set a world record by doing 1,000 push-ups in 23 minutes, still does push-ups as part of his daily workout. Now he balances his feet and each hand on three chairs.
"That way I can go way down, even lower than if I was on the floor," he said. "That's really tough."
· Intensity : Work out at 60% - 90% of your heart's maximum pumping capacity. Calculate by subtracting your age from 220 and then calculating 60% (for low intensity) - 90% (for high intensity) of this figure.
· Duration : 15 -60 minutes of continuous activity
· Mode : Any activity that involves large muscle groups in continuous movement eg running, walking, hiking, swimming, bicycling, rowing, rope skipping etc
Health Clubs & Gyms - Quick Tips
1.Before you join, think skeptically about what activities you are likely to participate in and how often you’ll be able to use the club. If you haven’t exercised before or for a long time, question whether you will be able to stick with a new fitness regimen. Most people who join clubs stop using them long before their memberships expire. Since most clubs charge nonrefundable initiation fees, and many clubs require or push annual contracts, you can waste a lot of money if you quit.
2.Consider whether you can get the exercise you want less expensively some other way—for example, by doing push-ups, sit-ups, and running on your own; by joining a sports team or exercise program; or by using a government-sponsored facility.
3.Shop. For roughly the same facilities, you might pay more than twice as much at some clubs as at others.
4.Be sure to press clubs you are considering for their best deals. When you are negotiating, get clubs to compete by mentioning other clubs you are considering. Many clubs have various fee plans and discount options and offer the best deals only if necessary to get the sale. Don’t allow sales staff to pressure you into making a decision. Check to see whether you qualify for a discounted rate due to an arrangement between your employer or health plan and the club. Find out about clubs’ rules on canceling a membership, selling a membership to someone else, and freezing a membership.
5.Try out any club you are considering by asking it for a guest pass to use. When you are there, check out the cleanliness and the condition of equipment, ask other members how crowded the club gets at hours when you might want to be there, and judge how helpful the staff is.
Stretching: The Truth
By Gretchen Reynolds : NY Times Article : November 2, 2008
When Duane Knudson, a professor of kinesiology at California State University, Chico, looks around campus at athletes warming up before practice, he sees one dangerous mistake after another. "They're stretching, touching their toes. . . . " He sighs. "It's discouraging."
If you're like most of us, you were taught the importance of warm-up exercises back in grade school, and you've likely continued with pretty much the same routine ever since. Science, however, has moved on. Researchers now believe that some of the more entrenched elements of many athletes' warm-up regimens are not only a waste of time but actually bad for you. The old presumption that holding a stretch for 20 to 30 seconds — known as static stretching — primes muscles for a workout is dead wrong. It actually weakens them. In a recent study conducted at the University of Nevada, Las Vegas, athletes generated less force from their leg muscles after static stretching than they did after not stretching at all. Other studies have found that this stretching decreases muscle strength by as much as 30 percent. Also, stretching one leg's muscles can reduce strength in the other leg as well, probably because the central nervous system rebels against the movements.
"There is a neuromuscular inhibitory response to static stretching," says Malachy McHugh, the director of research at the Nicholas Institute of Sports Medicine and Athletic Trauma at Lenox Hill Hospital in New York City. The straining muscle becomes less responsive and stays weakened for up to 30 minutes after stretching, which is not how an athlete wants to begin a workout.
THE RIGHT WARM-UP should do two things: loosen muscles and tendons to increase the range of motion of various joints, and literally warm up the body. When you're at rest, there's less blood flow to muscles and tendons, and they stiffen. "You need to make tissues and tendons compliant before beginning exercise," Knudson says.
A well-designed warm-up starts by increasing body heat and blood flow. Warm muscles and dilated blood vessels pull oxygen from the bloodstream more efficiently and use stored muscle fuel more effectively. They also withstand loads better. One significant if gruesome study found that the leg-muscle tissue of laboratory rabbits could be stretched farther before ripping if it had been electronically stimulated — that is, warmed up.
To raise the body's temperature, a warm-up must begin with aerobic activity, usually light jogging. Most coaches and athletes have known this for years. That's why tennis players run around the court four or five times before a match and marathoners stride in front of the starting line. But many athletes do this portion of their warm-up too intensely or too early. A 2002 study of collegiate volleyball players found that those who'd warmed up and then sat on the bench for 30 minutes had lower backs that were stiffer than they had been before the warm-up. And a number of recent studies have demonstrated that an overly vigorous aerobic warm-up simply makes you tired. Most experts advise starting your warm-up jog at about 40 percent of your maximum heart rate (a very easy pace) and progressing to about 60 percent. The aerobic warm-up should take only 5 to 10 minutes, with a 5-minute recovery. (Sprinters require longer warm-ups, because the loads exerted on their muscles are so extreme.) Then it's time for the most important and unorthodox part of a proper warm-up regimen, the Spider-Man and its counterparts.
"TOWARDS THE end of my playing career, in about 2000, I started seeing some of the other guys out on the court doing these strange things before a match and thinking, What in the world is that?" says Mark Merklein, 36, once a highly ranked tennis player and now a national coach for the United States Tennis Association. The players were lunging, kicking and occasionally skittering, spider-like, along the sidelines. They were early adopters of a new approach to stretching.
While static stretching is still almost universally practiced among amateur athletes — watch your child's soccer team next weekend — it doesn't improve the muscles' ability to perform with more power, physiologists now agree. "You may feel as if you're able to stretch farther after holding a stretch for 30 seconds," McHugh says, "so you think you've increased that muscle's readiness." But typically you've increased only your mental tolerance for the discomfort of the stretch. The muscle is actually weaker.
Stretching muscles while moving, on the other hand, a technique known as dynamic stretching or dynamic warm-ups, increases power, flexibility and range of motion. Muscles in motion don't experience that insidious inhibitory response. They instead get what McHugh calls "an excitatory message" to perform.
Dynamic stretching is at its most effective when it's relatively sports specific. "You need range-of-motion exercises that activate all of the joints and connective tissue that will be needed for the task ahead," says Terrence Mahon, a coach with Team Running USA, home to the Olympic marathoners Ryan Hall and Deena Kastor. For runners, an ideal warm-up might include squats, lunges and "form drills" like kicking your buttocks with your heels. Athletes who need to move rapidly in different directions, like soccer, tennis or basketball players, should do dynamic stretches that involve many parts of the body. "Spider-Man" is a particularly good drill: drop onto all fours and crawl the width of the court, as if you were climbing a wall. (For other dynamic stretches, see the sidebar below.)
Even golfers, notoriously nonchalant about warming up (a recent survey of 304 recreational golfers found that two-thirds seldom or never bother), would benefit from exerting themselves a bit before teeing off. In one 2004 study, golfers who did dynamic warm- up exercises and practice swings increased their clubhead speed and were projected to have dropped their handicaps by seven strokes over seven weeks.
Controversy remains about the extent to which dynamic warm-ups prevent injury. But studies have been increasingly clear that static stretching alone before exercise does little or nothing to help. The largest study has been done on military recruits; results showed that an almost equal number of subjects developed lower-limb injuries (shin splints, stress fractures, etc.), regardless of whether they had performed static stretches before training sessions. A major study published earlier this year by the Centers for Disease Control, on the other hand, found that knee injuries were cut nearly in half among female collegiate soccer players who followed a warm-up program that included both dynamic warm-up exercises and static stretching. (For a sample routine, visit www.aclprevent.com/pepprogram.htm.) And in golf, new research by Andrea Fradkin, an assistant professor of exercise science at Bloomsburg University of Pennsylvania, suggests that those who warm up are nine times less likely to be injured.
"It was eye-opening," says Fradkin, formerly a feckless golfer herself. "I used to not really warm up. I do now."
You're Getting Warmer: The Best Dynamic Stretches
These exercises- as taught by the United States Tennis Association's player-development program – are good for many athletes, even golfers. Do them immediately after your aerobic warm-up and as soon as possible before your workout.
STRAIGHT-LEG MARCH
(for the hamstrings and gluteus muscles)
Kick one leg straight out in front of you, with your toes flexed toward the sky. Reach your opposite arm to the upturned toes. Drop the leg and repeat with the opposite limbs. Continue the sequence for at least six or seven repetitions.
SCORPION
(for the lower back, hip flexors and gluteus muscles)
Lie on your stomach, with your arms outstretched and your feet flexed so that only your toes are touching the ground. Kick your right foot toward your left arm, then kick your leftfoot toward your right arm. Since this is an advanced exercise, begin slowly, and repeat up to 12 times.
HANDWALKS
(for the shoulders, core muscles, and hamstrings)
Stand straight, with your legs together. Bend over until both hands are flat on the ground. "Walk" with your hands forward until your back is almost extended. Keeping your legs straight, inch your feet toward your hands, then walk your hands forward again. Repeat five or six times. G.R.
Questions For Your Doctor : What to Ask About Exercise
By Marilynn Larkin : NY Times Article ; January 8, 2008
A new diagnosis can be a frightening experience, and ever-changing research can complicate already difficult treatment decisions. Here are some questions you might ask your doctor if exercise has been recommended as part of your treatment plan.
Why are you recommending exercise for my condition? I thought medication would be enough.
Physicians increasingly prescribe exercise as a complement to medication for a wide range of medical complaints, though it’s not a substitute for taking your drugs. Exercise may help slow progression of certain conditions, such as arthritis, Parkinson’s disease and chronic obstructive pulmonary disease, or improve other aspects of your health, including cardiovascular endurance and strength. Exercise can also boost mood and sense of well-being.
What kind of exercises should I do? Are there some I should avoid?
If you haven’t been exercising regularly, start by walking. And talk to your doctor first, especially if you’re over 50 or have a medical condition. He or she can recommend a physical therapist or other health professional with experience in your condition. A physical therapist can also show you how to add appropriate resistance and flexibility exercises to your routine.
Can medications affect my ability to exercise?
Some drugs may cause side effects like dizziness, so you want to be sure to choose exercises that allow you to stop and sit down if necessary. Other medications can affect heart rate, making it difficult to tell when you are exercising at or near your target heart rate.
Do I need to lose weight before I start?
Most people can embark on an exercise program regardless of weight. Begin by walking. If you can’t walk 30 minutes at a time, do shorter bouts. Exercising 10 minutes at a time, three times a day, confers similar benefits to exercising in a single 30-minute session, studies show. Increasing physical activity can also help minimize age-related weight gain.
I haven’t regularly exercised since college, and that was years ago. Can I really get benefits now?
You’re never too old to start, as the adage goes. In recent studies, people in their 70s and 80s demonstrated significant gains in strength and function from participation in a strength-training program. Older adults also get cardiovascular benefits from aerobic activity. Improving aerobic capacity and strength will make it easier to do everyday activities and allows older adults stay independent longer.
How do I get started?
Several Web-based programs can help you jump in, including the American Heart Association’s “Choose to Move” program and the “Exercise and Screening for You,” or EASY, tool from Texas A&M Health Science Center. Also see the American College of Sports Medicine’s brochure, Energy Expenditure in Different Modes of Exercise.
How much exercise should I do?
New exercise recommendations from the American College of Sports Medicine and the American Heart Association advise moderately intense aerobic exercise 30 minutes a day, five days a week, or vigorously intense aerobic exercise 20 minutes a day, three days a week. In addition, they recommend a mix of eight to 10 strength-training exercises -- on a schedule of 10 to 15 repetitions of each exercise two to three times per week for those with chronic ailments or people over 65.
Do I need to join a gym?
It’s not necessary to join a gym; all you need are a pair of athletic shoes and a little motivation. Some people find that exercising with a friend or in a group helps them stay on track.
Should I buy special equipment?
You don’t need special equipment. However, it may be helpful to invest in resistance bands or free weights to do resistance training. A stability ball to improve balance or a home exercise machine may also help. The American College of Sports Medicine offers brochures to help seniors and others make appropriate purchases and learn to use equipment properly.
I travel a lot for business. How can I keep up my exercise routine?
Know what fitness facilities are available at your hotel and in the immediate area. Plan exercise time around your business obligations. Be aware that the latest research suggests that you can take up to a week off from exercise without any significant reduction in your fitness level. During longer trips, focus on maintaining your fitness with some form of aerobic or strength training -- even though it might not be your usual routine --at least twice a week.
Post exercise recovery
By Gretchen Reynolds
NY Times Article : June 1, 2008
From the perspective of an athlete, few things top the virtuous satisfaction that comes from a hard workout. That 10-mile run, that 1,500-meter pool sprint, that hour with the free weights. Makes you feel great, right? You'll do it again tomorrow, for sure. But then it hits — the aftermath.
Within a few hours, your muscles begin sending vicious little reminders about your impressive efforts. Delayed-onset muscle soreness, as it's called, settles in roughly 12 to 24 hours after an intense bout of training, especially if it involved unfamiliar or extreme movements. The affected muscles become so tender and strained that the process of rising from bed the next morning becomes a challenge.
Even if you haven't arrived at this sorry state, repeated hard workouts can tax the body in insidious ways. Muscles, over the course of an hour or so of serious work, use up most of their stored energy. Without remediation, those muscles won't respond as well during your next workout. They'll be more prone to injury. You'll be slower. The 70-year-old from down the street will pass you on the running path.
Completing a hard workout, then, is just the first step. You also have to undo all the damage you've just done.
Start with your postworkout meal. The regeneration of your muscles begins, improbably as it may seem, with that. "Back in the early '90s, most athletes, especially runners and cyclists, were preoccupied with carbohydrates," says John Ivy, the chairman of the department of kinesiology and health education at the University of Texas in Austin and one of the pioneers of research into exercise recovery. This was in the heyday of carbo-loading, when athletes were convinced that the more pasta and bread they ate before a hard workout, the more stored energy they'd have.
But carbo-loading in advance of exercise is not the most efficient way to stock muscles with fuel, physiologists now know, thanks in large part to research conducted by Ivy. When reviewing studies of diabetics, he became intrigued by similarities with his own tests on cyclists: for both groups, insulin in the blood was more effective at carrying energy into the muscles if those muscles had recently been active. "Exercise makes your muscles more responsive to insulin, and this insulin, in turn, increases glycogen muscle uptake," he says. In other words, exercise prompts your muscles to absorb more fuel — glucose, which is stored as glycogen — from the bloodstream. (Carbo-loading can't take advantage of this insulin response because it precedes, rather than follows, a workout.) Your body is actually primed by the exercise to help itself replenish lost fuel.
This improved insulin response, however, lasts only for a brief time after a workout. "You have a window of about 30 to 45 minutes," Ivy says. After that, muscles become resistant to insulin and much less able to absorb glucose. Drinking or eating carbohydrates immediately after a strenuous workout, at a level of at least one gram per kilogram of body weight, is therefore essential to restoring the glycogen you've burned. Wait even a few hours and your ability to replenish that fuel drops by half.
It's also crucial that you take in some protein. Though it poses challenges to strict vegetarians, the latest research shows quite definitively that protein spurs even more of an insulin response than do exercise and carbohydrates alone. "Protein co-ingestion can accelerate muscle glycogen repletion by stimulating endogenous insulin release," says Luc van Loon, an associate professor of human movement sciences at Maastricht University in the Netherlands and the author of several important studies about recovery. Translation: coupling protein with carbohydrates prompts your muscles to store even more glycogen for use during your next workout.
"I'd advise people to have their recovery drink ready and waiting for them before they leave on a run or long bike ride," Ivy says. Ivy himself often drinks low-fat chocolate milk, but any food or drink that includes both carbohydrates and protein — a recovery drink, a smoothie, yogurt — will work.
Then have a real meal within two hours. "You can maintain increased insulin levels and accelerated rates of recovery for about four to six hours if you continue eating," Ivy says. Of course, you can also get by without such diet timing. "But you won't recover as well," Ivy continues. "You probably won't be able to work out as hard on a daily basis." The old guy who chugs his milk and Hershey's syrup will not only pass you — he'll lap you.
Meanwhile, there's the physical damage inside your muscles to consider. Skeletal muscle is a unique kind of tissue, made up of long, thin fibers composed of several different proteins. These proteins interlock like Legos inside fibrous compartments called sarcomeres. Sarcomeres can stretch, but only so far.
During certain kinds of movements, some sarcomeres are pulled past their tolerance. The proteins inside separate, resulting in micro-tears throughout your muscle tissue. After a few hours, this leads to inflammation, swelling, stiffness and pain. (Eccentric muscle contractions, which lengthen muscles, are the main culprit in delayed-onset muscle soreness. Concentric contractions, in which muscles shorten — the upward motion of a biceps curl, for instance — cause less damage. That's why running downhill makes you more sore the next day than running on flat ground.)
"This soreness is actually a good thing," says Thomas Swensen, a professor of exercise and sports science at Ithaca College in Ithaca, N.Y., and a leading researcher into exercise recovery. "You want to stress the muscles. They will adapt positively." The muscles will rebuild themselves, becoming stronger and more pliable. "That's the whole point of hard training," he says. "But it's only effective if you recover fully."
Which is another reason it's important to up your protein intake after a workout; that same protein will also help speed muscle repair. "Exercise stimulates muscle protein synthesis and protein breakdown," van Loon says. "However, without protein or amino acid ingestion, the net balance between protein synthesis and breakdown will remain negative" — i.e., your workouts, in the long run, may do your muscles more harm than good. But eat enough protein immediately after exercising and your muscles will repair themselves fully and become stronger.
Other postworkout recovery strategies, including many that athletes swear by, have far less scientific backing. Take massage. A 2000 study of British boxers showed that postworkout massage made the athletes only feel as if they were recovering quickly; they did not perform any better than those not massaged. Swensen's own 2003 study of massage and recovery produced similar results as the British research.
These studies, however, like many others that have examined massage and exercise, were small and short-term. "It's possible that if you followed athletes over the course of several months," Swensen says, "you might see some benefits from massage. Those studies haven't been done."
Similar ambiguity clouds the use of ibuprofen after exercise. Although advertised as an anti-inflammatory, ibuprofen doesn't always work as expected. A 2006 study of the drug's use among ultra-marathoners found that it did not lessen muscle damage or soreness or reduce inflammation. And although most users do not experience side effects, ibuprofen has been associated with kidney damage and gastrointestinal bleeding.
Finally, there are ice and heat. Many elite athletes swear by a limb-numbing ice bath, and others prefer a soak in a hot tub — although little scientific evidence supports either remedy. Ice will effectively block the swelling associated with a serious injury, such as a sprain, but has not been proven to speed the healing of muscle tissue stressed by a workout. In a study published last year in the British Journal of Sports Medicine, people treated with ice after strenuous exercise later reported more pain upon standing than people immersed in tepid water. The study's authors bluntly concluded that their research "challenges the wide use of [icing] as a recovery strategy by athletes." Similarly, a study published in March in the European Journal of Applied Physiology found that, when it came to muscle recovery, a hot bath was little better than merely sitting quietly for a while.
So where does that leave you, the athlete who has just worked out so diligently? Mixing a smoothie or glass of chocolate milk, the one recovery strategy that satisfies both your inner physiologist and inner child. .
Exercise
Exercise for life.
- What is cardiovascular exercise?
- What is my target heart rate?
- Should I do strength training?
- How can I build flexibility?
- Is there a program just right for me?
- How can I prevent injury?
Before you start an exercise program
If you have decided to start an exercise program, you are already on your way to a healthier heart and a fitter body. The first step you should take is to see your doctor, especially if you have any of the health risks listed below:
- You are taking a prescription medicine.
- You have ever had any kind of heart problem, especially a heart attack.
- You have diabetes.
- You have problems with your bones or joints.
- You have high blood pressure and do not take medicine for it.
- You have a family history of coronary artery disease.
- You are a man over 45 or a woman over 50, and you are not used to doing even moderate levels of exercise.
- You smoke.
- You are very overweight.
There are 3 categories of exercises: cardiovascular, strength-building, and flexibility.
Cardiovascular exercise is also known as aerobic exercise. Aerobic exercise uses your large muscles and can be continued for long periods. For example, walking, jogging, swimming, and cycling are aerobic activities. These types of exercises drive your body to use oxygen more efficiently and deliver maximum benefits to your heart, lungs, and circulatory system.
Strength-building and flexibility exercises are known as anaerobic exercise. Anaerobic exercise does not have cardiovascular benefits, but it makes your muscles and bones stronger. Strength-building exercises require short, intense effort. Flexibility exercises, which are also anaerobic, tone your muscles through stretching and can prevent muscle and joint problems later in life.
A well-balanced exercise program should include some type of exercise from each category.
Cardiovascular Exercise
A simple definition of cardiovascular exercise is any exercise that raises your heart rate to a level where you can still talk, but you start to sweat a little.
At least 20 minutes of cardiovascular exercise 3 or 4 days a week should be enough to maintain a good fitness level. Any movement is good, even house or yard work. But if your goal is to lose weight, you will need to do some form of cardiovascular exercise for 4 or more days a week for 30 to 45 minutes or longer.
The ideal cardiovascular exercise program starts with a 5- to 10-minute warm-up, which includes gentle movements that will slightly increase your heart rate.
Then, slowly move into 20 or more minutes of a cardiovascular exercise of your choice, such as aerobics, jogging on a treadmill, or walking, to reach what is called your target heart rate. (The chart below can help you find your target heart rate zone.) Your target heart rate is a guideline that can help you measure your fitness level before the start of your program and help you keep track of your progress after you begin an exercise program. Target heart rate also lets you know how hard you are exercising. If you are beginning an exercise program, you should aim for the low end of your target heart rate zone. If you exercise regularly, you may want to work out at the high end of the zone.
To stay within your target heart rate zone, you will need to take your pulse every so often as you exercise. You can find your pulse in 2 places: at the base of your thumb on either hand (called the radial pulse), or at the side of your neck (called the carotid pulse). Put your first 2 fingers over your pulse and count the number of beats within a 10-second period. Multiply this number by 6, and you will have the number of heartbeats in a minute. For example, if you counted your pulse to be 20 during the 10-second pulse count, your heart rate would be 120 beats per minute.
Note: If you are taking certain medicines, like beta blockers, you may not be able to reach your target heart rate. Remember, always have your doctor's approval before beginning any exercise program.
You never want to begin exercising by immediately reaching your target heart rate, because your muscles and circulatory system need to warm up slowly. Intensify your activity slowly during exercise until you reach your target heart rate. There is no need to exceed your target heart rate during exercise.
End your exercise program with a 5- to 10-minute cool down, which will help to lower your heart rate and prevent your muscles from tightening up.
Strength-Building Exercise
People who lift weights or who use any type of equipment that requires weights are doing strength-building exercise. Strength-building exercise makes your muscles and bones stronger and increases your metabolism. Strength exercises also make your muscles larger. Your muscles use calories for energy even when your body is at rest. So, by increasing your muscle mass, you are burning more calories all of the time. If you strength train regularly, you will find that your body looks leaner and you will lose fat.
Strength-building exercises should be performed 2 to 3 times a week for best results. Always warm up your muscles for 5 to 10 minutes before you begin lifting any type of weight or before performing any resistance exercises.
Find a weight that you can comfortably lift for between 8 and 12 repetitions (reps). Reps are the number of times the exercise is performed. When you can easily do 12 to 15 reps of an exercise, it is time to increase the amount of weight you are lifting.
You should choose exercises that work your legs, arms, chest, back, and stomach. Make sure that each movement is performed in a slow, controlled way. Do not jerk the weights or use too much force.
Also, do not hold your breath during the movements. Remember to breathe out as you lift the weight and breathe in as you lower the weight.
Flexibility Exercises
Flexibility exercises are the most neglected part of a fitness program. Having flexibility can improve your posture, reduce your risk of injury, give you more freedom of movement, and release muscle tension and soreness.
Before you start the stretching phase of your program, always do 5 to 10 minutes of warm-up to loosen your muscles. Stretching cold muscles can lead to injury. Some examples of a warm-up are walking around, marching in place, slowly riding an exercise bike, or lightly jogging. If stretching is part of a longer program that includes a cardiovascular workout, always stretch after the cool-down section of your program. You want to make sure that your heart rate has slowed before you begin the stretching phase.
You should try to do stretching exercises for each muscle group. Each stretch should be done slowly and held for at least 10 to 30 seconds.
Do not bounce while you stretch, because bouncing can injure your muscles. Also, do not over stretch a muscle, because it can cause strain or even a tear. Try not to hold your breath while you stretch. Instead, take long, deep breaths throughout your stretching program.
Choosing the right program
Whether you decide to join a health club or to exercise on your own, you will make exercise a regular part of your life if you like doing it. So try to find one or more activities that you like to do or that give you satisfaction. Remember that exercise does not have to feel like a strenuous workout. Your body benefits from any type of movement. So if running or weight lifting are not for you, think about an activity like tai chi or yoga.
If you decide to join a group exercise program like an aerobics class or water-fitness class, here are some tips for choosing a program:
- Choose an instructor whom you like and feel comfortable with. You should be able to ask your instructor about any part of the fitness program.
- Find a program that meets your exercise needs and goals. That sounds simple enough, but a lot of people do not have a clear picture of what they hope to gain from exercise. For example, to help you lose weight, you need to burn calories through aerobic activity. But to build muscle, you will need to work specific muscle groups.
- Choose an instructor who can show you how to exercise safely and properly. Your instructor should be able to tell you what muscle groups each exercise works. The instructor should also show the class the different levels in which each exercise can be done, so each person in your class can modify the activity to meet his or her fitness level.
- Choose an instructor who is certified by a nationally recognized certification program.
- Ask the trainer to give you a list of references. Other clients are one of the best ways to find out if this is the trainer for you.
- Make sure that the trainer has a schedule that works with yours. It is easier to fit exercise into your life if you set aside the same time each day or week for training and for exercise.
- Choose a trainer who is certified by a nationally recognized certification program.
Preventing exercise injuries
One of the most important parts of an exercise program is the warm-up, but most people do not take the time to warm up properly.
A warm up increases your body temperature and makes your muscles loose and ready to exercise. Marching in place, walking for a few minutes, doing some jumping jacks, or jogging in place are all ways to get the blood flowing to the muscles and to prepare them for exercise.
These same exercises can and should be done to cool down after you exercise.
Buying good shoes before you begin an exercise program is one of the most important ways to make sure that you do not get hurt. Your shoes not only protect your feet but also give you a cushion for the weight of your whole body. That is why it is so important that your shoes fit properly.
You should go shoe shopping at the end of the day, when your foot is at its largest size. When you try on a shoe, there should be one-half inch between the end of your toe and the end of the shoe, and your foot should not slip or slide around inside.
Your shoes should feel good when you buy them, and they should not need a "breaking-in" period. If you are exercising regularly, you will most likely need to buy new shoes about every 3 to 6 months. Shoes that are used regularly lose the ability to absorb your weight during exercise and may cause injury to your knees and ankles.
If you are new to an exercise program, and you are exercising at a health club or fitness facility, ask for help before you try something new. The staff should be able to show you how to work any exercise equipment that you do not know how to use. Asking for help will stop you from lifting too much weight or from using the wrong posture when you use the machine. This, in turn, leads to fewer injuries.
Finally, use your good judgment and stay within your exercise limits. Light exercise performed regularly is always better than one gut-wrenching workout session a week. Your body will tell you if you are pushing it too hard. Pain, dizziness, fainting, a cold sweat, or pale skin are signs to stop. Even professional athletes and coaches will tell you that physical fitness is gained a little at a time.
Remember that exercise is not limited to working out in a health club or jogging around a track. Pushing a lawn mower, putting up storm windows, and vacuuming a rug are all forms of exercise, although they are not cardiovascular exercise. If you do not have a job that requires physical activity, taking the stairs instead of the elevator, parking farther away from your office, or taking a brief walk at lunch are all ways to find fitness during your day.
Exercise...Exercise....Exercise
By Jane E. Brody : NY Times Article : December 19, 2006
An apology to all baby boomers and beyond: I’m afraid that in our efforts to get everyone to become physically active, we’ve sold you a bill of goods. A 30-minute walk on most days is just not enough. There is much more to becoming — and staying — physically fit as you age than engaging in regular aerobic activity. (Of course, the same applies to those younger than 60.)
In addition to activities like walking, jogging, cycling and swimming that promote endurance, cardiovascular health and weight control, there is a dire need for exercises that improve posture and increase strength, flexibility and balance. These exercises can greatly reduce the risk of injuries from sports and endurance activities, the demands of daily life, falls and other accidents.
Musculoskeletal injuries are now the No. 1 one reason for seeking medical care in the United States. And falls, the Centers for Disease Control and Prevention reported last month, have become the leading cause of injury deaths for men and women 65 and older.
Unless you do something to slow the deterioration in muscle, bone strength and agility that naturally accompanies aging, you will become a prime candidate for what Dr. Nicholas A. DiNubile, an orthopedic surgeon at the Hospital of the University of Pennsylvania, calls “boomeritis.”
“By their 40th birthday, people often have vulnerabilities — weak links — and as the first generation that is trying to stay active in droves, baby boomers are pushing their frames to the breakpoint,” Dr. DiNubile said in introducing a November press event in New York sponsored by the American Academy of Orthopedic Surgeons and the National Athletic Trainers’ Association.
“Baby boomers are falling apart — developing tendinitis, bursitis, arthritis and ‘fix-me-itis,’ the idea that modern medicine can fix anything,” he said. “It’s much better to prevent things than to have to try to fix them.”
Dr. DiNubile pointed out that evolution had not kept up with the doubling of the human life span in the last 100 years. To counter the inevitable declines with age, we have to provide our bodies with an extended warranty.
Assess Your Fitness
In their recently published book, “Age-Defying Fitness” (Peachtree Publishers), two prominent physical therapists, Marilyn Moffat of New York University and Carole B. Lewis of Washington, D.C., provide the ingredients to help you make the most of your body for the rest of your life: a quick quiz and a five-part test to assess the status of your posture, strength, balance, flexibility and endurance, followed by five chapters with step-by-step instructions on how to safely improve the areas in which you are lacking.
The therapists describe what happens to these “five domains of fitness” as you age. Posture begins changing as early as the teenage years, the result of activities like prolonged sitting, carrying a heavy purse or briefcase, or working at a computer.
Strength declines as muscle fibers decrease in size and number and as the supply of nerve stimulation and energy to the muscles diminishes. Balance deteriorates as muscles tighten and weaken and joints lose their full range of motion.
Flexibility declines because connective tissue throughout the body becomes less elastic. And endurance falls off because of reduced flexibility, weakened muscles, and stiffer lungs and blood vessels.
Still not convinced you need to work on your fitness? See how you do on the therapists’ quiz:
- Are you not standing as straight and tall as you once did?
- Is walking up a flight of stairs a strain at times?
- Are you getting up from a chair more slowly than you used to?
- Is it getting harder to look to the left and right while backing up?
- Do you get stiff sitting through a long movie?
- Is standing on one leg to put on your shoe difficult or impossible?
- Do you trip or lose your balance more easily?
- Does walking or jogging a distance take longer than it used to?
“The antidote to aging is activity,” the therapists wrote. “Inactivity magnifies age-related changes, but action maintains and increases your abilities in all five domains.”
No Time to Waste
Dr. Vonda J. Wright, a sports medicine specialist at the University of Pittsburgh Medical Center, said at the New York meeting that “boomers are 59, and we must intervene now to head off what happens to those who age in a sedentary way.”
Injury and arthritis are the main reasons people stop exercising, she said. She urged those in need of a joint replacement not to postpone the surgery, which she likened to repairing a pothole.
Marjorie J. Albohm, a certified athletic trainer affiliated with OrthoIndy and the Indiana Orthopedic Hospital in Indianapolis, cautioned against “cookbook recipes” for exercise. “The key to a good workout is customization,” based on a professional assessment of flexibility, cardiovascular endurance, strength and balance, she said. “The goal is to minimize symptoms and prevent new injuries,” Ms. Albohm said, and she urged people to listen to their bodies to avoid making things worse.
Ms. Albohm emphasized flexibility, saying it is “not optional” as you age. “To prevent stiffness and maintain joint mobility you should stretch daily for 15 to 20 minutes,” she said “using slow, controlled movements, before or after your exercise program.”
For cardiovascular endurance, she recommended alternating between weight-bearing (walking, jogging) and non-weight-bearing (swimming, cycling) aerobic activities three days a week for 30 to 45 minutes each time.
Muscle strength, Ms. Albohm noted, can be increased at any age, even in one’s 90s, to protect against falls, maintain mobility, prevent new injuries and empower individuals. Especially important is strengthening the muscles in the front and sides of the thighs, which help support the knees, and strengthening core muscles of the trunk (back, buttocks and abdomen) to protect the spine and support the entire body.
Finally, we need to worry about our bones. At least 1.5 million “fragility fractures” occur annually in the United States. These are breaks that result when someone falls from a standing height or less, trips over the cat or lifts something heavy, and they affect men as well as women, Dr. Laura Tosi, an orthopedic surgeon at Children’s National Medical Center in Washington, D.C., said at the New York event.
“A history of a fragility fracture is far more predictive of future fractures than a bone density test,” Dr. Tosi said, adding that a major cause is a shortage of vitamin D, which lets calcium into bones.
“The current standard for vitamin D is not adequate,” she said, and predicted it would soon be raised to perhaps 1,000 International Units a day. Vitamin supplements are crucial, because adequate amounts of vitamin D cannot be absorbed through diet and sunshine alone.
Personal Health: You Name It and Exercise Helps It
By Jane E. Brody
NY Times Article : April 28, 2008
Randi considers the Y.M.C.A. her lifeline, especially the pool. Randi weighs more than 300 pounds and has borderline diabetes, but she controls her blood sugar and keeps her bright outlook on life by swimming every day for about 45 minutes.
Randi overcame any self-consciousness about her weight for the sake of her health, and those who swim with her and share the open locker room are proud of her. If only the millions of others beset with chronic health problems recognized the inestimable value to their physical and emotional well-being of regular physical exercise.
“The single thing that comes close to a magic bullet, in terms of its strong and universal benefits, is exercise,” Frank Hu, epidemiologist at the Harvard School of Public Health, said in the Harvard Magazine.
I have written often about the protective roles of exercise. It can lower the risk of heart attack, stroke, hypertension, diabetes, obesity, depression, dementia, osteoporosis, gallstones, diverticulitis, falls, erectile dysfunction, peripheral vascular disease and 12 kinds of cancer.
But what if you already have one of these conditions? Or an ailment like rheumatoid arthritis, multiple sclerosis, Parkinson’s disease, congestive heart failure or osteoarthritis? How can you exercise if you’re always tired or in pain or have trouble breathing? Can exercise really help?
You bet it can. Marilyn Moffat, a professor of physical therapy at New York University and co-author with Carole B. Lewis of “Age-Defying Fitness” (Peachtree, 2006), conducts workshops for physical therapists around the country and abroad, demonstrating how people with chronic health problems can improve their health and quality of life by learning how to exercise safely.
Up and Moving
“The data show that regular moderate exercise increases your ability to battle the effects of disease,” Dr. Moffat said in an interview. “It has a positive effect on both physical and mental well-being. The goal is to do as much physical activity as your body lets you do, and rest when you need to rest.”
In years past, doctors were afraid to let heart patients exercise. When my father had a heart attack in 1968, he was kept sedentary for six weeks. Now, heart attack patients are in bed barely half a day before they are up and moving, Dr. Moffat said.
The core of cardiac rehab is a progressive exercise program to increase the ability of the heart to pump oxygen- and nutrient-rich blood more effectively throughout the body. The outcome is better endurance, greater ability to enjoy life and decreased mortality.
The same goes for patients with congestive heart failure. “Heart failure patients as old as 91 can increase their oxygen consumption significantly,” Dr. Moffat said.
Aerobic exercise lowers blood pressure in people with hypertension, and it improves peripheral circulation in people who develop cramping leg pains when they walk — a condition called intermittent claudication. The treatment for it, in fact, is to walk a little farther each day.
In people who have had transient ischemic attacks, or ministrokes, “gradually increasing exercise improves blood flow to the brain and may diminish the risk of a full-blown stroke,” Dr. Moffat said. And aerobic and strength exercises have been shown to improve endurance, walking speed and the ability to perform tasks of daily living up to six years after a stroke.
As Randi knows, moderate exercise cuts the risk of developing diabetes. And for those with diabetes, exercise improves glucose tolerance — less medication is needed to control blood sugar — and reduces the risk of life-threatening complications.
Perhaps the most immediate benefits are reaped by people with joint and neuromuscular disorders. Without exercise, those at risk of osteoarthritis become crippled by stiff, deteriorated joints. But exercise that increases strength and aerobic capacity can reduce pain, depression and anxiety and improve function, balance and quality of life.
Likewise for people with rheumatoid arthritis. “The less they do, the worse things get,” Dr. Moffat said. “The more their joints move, the better.”
Exercise that builds gradually and protects inflamed joints can diminish pain, fatigue, morning stiffness, depression and anxiety, she said, and improve strength, walking speed and activity.
Exercise is crucial to improving function of total hip or knee replacements. But “most patients with knee replacements don’t get intensive enough activity,” Dr. Moffat said.
Water exercises are particularly helpful for people with multiple sclerosis, who must avoid overheating. And for those with Parkinson’s, resistance training and aerobic exercise can increase their ability to function independently and improve their balance, stride length, walking speed and mood.
Resistance training, along with aerobic exercise, is especially helpful for people with chronic obstructive pulmonary disease; it helps counter the loss of muscle mass and strength from lack of oxygen.
In the February/March issue of ACE Certified News, Natalie Digate Muth, a registered dietitian and personal trainer, emphasized the value of a good workout for people suffering from depression. Mastering a new skill increases their sense of worth, social contact improves mood, and the endorphins released during exercise improve well-being.
“Exercise is an important adjunct to pharmacological therapy, and it does not matter how severe the depression — exercise works equally well for people with moderate or severe depression,” wrote Ms. Muth, who is pursuing a medical degree at the University of North Carolina, Chapel Hill.
Feel-Good Hormones
Healthy people may have difficulty appreciating the burdens faced by those with chronic ailments, Dr. Nancey Trevanian Tsai noted in the same issue of ACE Certified News. “Oftentimes, disease-ridden statements — like ‘I’m a diabetic’ — become barricades that keep clients from seeing themselves getting better,” she said, and many feel “enslaved by their diseases and treatments.”
But the feel-good hormones released through exercise can help sustain activity.
“With regular exercise, the body seeks to continue staying active,” wrote Dr. Tsai, an assistant professor of neurosciences at the Medical University of South Carolina in Charleston. She recommended an exercise program tailored to the person’s current abilities, daily needs, medication schedule, side effects and response to treatment.
She urged trainers who work with people with chronic ailments to start slowly with easily achievable goals, build gradually on each accomplishment and focus on functional gains. Over time, a sense of accomplishment, better sleep, less pain and enhanced satisfaction with life can become further reasons to pursue physical activity.
“Even if exercise is tough to schedule,” Dr. Moffat said, “you feel so much better, it’s crazy not to do it.”
Rest and Motion. The value of interval training
By Peter Jaret : NY Times article : May 3, 2007
Some gym goers are tortoises. They prefer to take their sweet time, leisurely pedaling or ambling along on a treadmill. Others are hares, impatiently racing through miles at high intensity.
Each approach offers similar health benefits: lower risk of heart disease, protection against Type 2 diabetes, and weight loss.
But new findings suggest that for at least one workout a week it pays to be both tortoise and hare — alternating short bursts of high-intensity exercise with easy-does-it recovery.
Weight watchers, prediabetics and those who simply want to increase their fitness all stand to gain.
This alternating fast-slow technique, called interval training, is hardly new. For decades, serious athletes have used it to improve performance.
But new evidence suggests that a workout with steep peaks and valleys can dramatically improve cardiovascular fitness and raise the body’s potential to burn fat.
Best of all, the benefits become evident in a matter of weeks.
“There’s definitely renewed interest in interval training,” said Ed Coyle, the director of the human performance laboratory at the University of Texas at Austin.
A 2005 study published in the Journal of Applied Physiology found that after just two weeks of interval training, six of the eight college-age men and women doubled their endurance, or the amount of time they could ride a bicycle at moderate intensity before exhaustion.
Eight volunteers in a control group, who did not do any interval training, showed no improvement in endurance.
Researchers at McMaster University in Hamilton, Ontario, had the exercisers sprint for 30 seconds, then either stop or pedal gently for four minutes.
Such a stark improvement in endurance after 15 minutes of intense cycling spread over two weeks was all the more surprising because the volunteers were already reasonably fit. They jogged, biked or did aerobic exercise two to three times a week.
Doing bursts of hard exercise not only improves cardiovascular fitness but also the body’s ability to burn fat, even during low- or moderate-intensity workouts, according to a study published this month, also in the Journal of Applied Physiology. Eight women in their early 20s cycled for 10 sets of four minutes of hard riding, followed by two minutes of rest. Over two weeks, they completed seven interval workouts.
After interval training, the amount of fat burned in an hour of continuous moderate cycling increased by 36 percent, said Jason L. Talanian, the lead author of the study and an exercise scientist at the University of Guelph in Ontario. Cardiovascular fitness — the ability of the heart and lungs to supply oxygen to working muscles — improved by 13 percent.
It didn’t matter how fit the subjects were before. Borderline sedentary subjects and the college athletes had similar increases in fitness and fat burning. “Even when interval training was added on top of other exercise they were doing, they still saw a significant improvement,” Mr. Talanian said.
That said, this was a small study that lacked a control group, so more research would be needed to confirm that interval training was responsible.
Interval training isn’t for everyone. “Pushing your heart rate up very high with intensive interval training can put a strain on the cardiovascular system, provoking a heart attack or stroke in people at risk,” said Walter R. Thompson, professor of exercise science at Georgia State University in Atlanta.
For anyone with heart disease or high blood pressure — or who has joint problems such as arthritis or is older than 60 — experts say to consult a doctor before starting interval training.
Still, anyone in good health might consider doing interval training once or twice a week. Joggers can alternate walking and sprints. Swimmers can complete a couple of fast laps, then four more slowly.
There is no single accepted formula for the ratio between hard work and a moderate pace or resting. In fact, many coaches recommend varying the duration of activity and rest.
But some guidelines apply. The high-intensity phase should be long and strenuous enough that a person is out of breath — typically one to four minutes of exercise at 80 to 85 percent of their maximum heart rate. Recovery periods should not last long enough for their pulse to return to its resting rate.
Also people should remember to adequately warm up before the first interval. Coaches advise that, ideally, people should not do interval work on consecutive days. More than 24 hours between such taxing sessions will allow the body to recover and help them avoid burnout.
What is so special about interval training? One advantage is that it allows exercisers to spend more time doing high-intensity activity than they could in a single sustained effort. “The rest period in interval training gives the body time to remove some of the waste products of working muscles,” said Barry A. Franklin, the director of the cardiac rehabilitation and exercise laboratories at the William Beaumont Hospital in Royal Oak, Mich.
To go hard, the body must use new muscle fibers. Once these recent recruits are trained, they are available to burn fuel even during easy-does-it workouts. “Any form of exercise that recruits new muscle fibers is going to enhance the body’s ability to metabolize carbohydrates and fat,” Dr. Coyle said.
Interval training also stimulates change in mitochondria, where fuel is converted to energy, causing them to burn fat first — even during low- and moderate-intensity workouts, Mr. Talanian said.
Improved fat burning means endurance athletes can go further before tapping into carbohydrate stores. It is also welcome news to anyone trying to lose weight or avoid gaining it.
Unfortunately, many people aren’t active enough to keep muscles healthy. At the sedentary extreme, one result can be what Dr. Coyle calls “metabolic stalling” — carbohydrates in the form of blood glucose and fat particles in the form of triglycerides sit in the blood. That, he suspects, could be a contributing factor to metabolic syndrome, the combination of obesity, insulin resistance, high cholesterol and elevated triglycerides that increases the risk of heart disease and diabetes.
The Benefits of lifting weights
By Judy Foreman : Boston Globe Article : January 21, 2008
I'm an exercise junkie - and proud of it. I swim, I run, I bike.
But, like many other people, I'm a disaster when it comes to lifting weights, also called strength, or resistance, training. The closest I come is lifting a few tiny dumbbells at home in front of the TV. And that's only when the Red Sox are on.
This is about to change, and not just because of lingering New Year's resolutions.
A growing body of evidence shows that strength training not only provides many benefits that aerobic workouts alone cannot, but also offers some of the same health benefits as aerobic conditioning.
It's long been known that weight lifting becomes more important as you get older to prevent injury and preserve the strength to do normal things like climbing stairs, hauling groceries, and chasing grandchildren.
What's comparatively new is that it does much more than that, potentially reducing the risk of developing heart disease, relieving neck pain, improving balance, and making it easier to battle the bulge - though it needs to be done properly to avoid injury.
The evidence for the value of strength training has grown so much that last year, the American College of Sports Medicine and the American Heart Association issued new recommendations for healthy adults 65 and older that stressed the importance of weight lifting.
The groups now recommend that all older Americans do eight to 10 repetitions for each of the major muscle groups (biceps, quadriceps, hamstrings, etc.). Resistance exercises should be done on two or more nonconsecutive days of the week.
The idea is to lift a weight that's heavy enough to work each muscle group until it is fatigued, so the amount you lift will increase as your strength grows. Weight-bearing exercise, like walking or running, does not count as weight lifting - that means you really have to lift weights or work out on a resistance machine.
One of the biggest benefits of strength training is that it dramatically increases muscle mass, which aerobic exercise does not, noted William J. Evans, director of the Nutrition, Metabolism, and Exercise Laboratory at the University of Arkansas for Medical Sciences. More muscle mass is good not just because it makes you stronger but because it increases basal metabolic rate - muscle cells even at rest burn more calories than fat cells.
Moreover, while aerobic exercise can significantly, although temporarily, increase blood pressure, a potential concern for some heart patients, resistance training does so only minimally, Evans said. Weight training also gets results fast - it only takes resistance training twice a week for a few weeks to begin to see a significant effect, compared with three days a week with aerobics.
Indeed, the more researchers probe the benefits of weight training for specific conditions, the stronger the case they can make, said Miriam Nelson, director of the John Hancock Center for Physical Activity and Nutrition at Tufts University.
Although studies have not yet proven that strength training lowers the risk of osteoporosis, Nelson said, they do show it lowers the risk of fractures by improving balance, bone density, and muscle mass. Weight training is also good for people with arthritis, she said, because stronger muscles can take the pressure off inflamed joints.
Weight training has been shown to have other benefits, too.
Research by Steven N. Blair, an exercise scientist at the University of South Carolina, suggests that people with greater muscle strength may be somewhat less likely to develop metabolic syndrome, a cluster of factors that raise the risk of heart disease and diabetes, such as increased waist size, high fasting blood sugar, high triglycerides, low HDL or "good" cholesterol, and high blood pressure. More studies are needed to confirm this association.
For older people with physical disabilities, 66 trials reviewed by Cochrane Collaboration, an international nonprofit group that evaluates health treatments, increasing strength and, to a lesser extent, function. A different 2007 Cochrane review of 34 studies showed that exercises, including strength training, can improve balance in women age 75 and older. Yet another 2007 Cochrane review of 34 studies on fibromyalgia (musculoskeletal pain) showed strength training may improve physical capacity.
And a Danish study just published last week showed that strength training can diminish the chronic neck pain of at computers.
I could go on. But I'm convinced. Weight training may not be as much fun as a run in the park. But I need it. I'm guessing you do, too.
The value of resistance training and the heart
While conventional wisdom once held that people with heart disease should not pump iron, a new scientific statement from the American Heart Association says some resistance training can be good for them.
"Just like we once learned that people with heart disease benefited from aerobic exercise, we are now learning that guided, moderate weight training also has significant benefits," said Mark Williams, professor of medicine at Creighton University School of Medicine in Omaha, Nebraska.
Weight training is seen as a complement to aerobic exercise, not a replacement, he said. But it provides everyday benefits.
"It helps people better perform tasks of daily living -- like lifting sacks of groceries," Williams said in a statement.
Resistance training is not recommended for people with certain conditions such as unstable heart disease, uncontrolled high blood pressure or heart rhythm disorders, infections in and around the heart, and some other serious problems.
The statement's recommendations for an initial weight-lifting program says resistance training should be performed:
- in a rhythmical manner at a moderate-to-slow controlled speed;
- through a full range of motion, avoiding breath-holding and straining by exhaling during the contraction or exertion phase of the lift and inhaling during the relaxation phase;
- alternating between upper and lower body work, to allow for adequate rest between exercises.
And they are easier to stick to.
"For people with cardiovascular disease, the level of resistance should be reduced and number of repetitions increased, resulting in a lower relative effort and reducing the likelihood of breath-holding and straining," the statement reads.
The heart benefits of weight training include increased muscle mass which can help in weight control.
"Patients who have had cardiac events are often apprehensive about returning to this type of activity, or doing things in their daily lives that might be perceived as strenuous ... Now we know that they can return to the active things they enjoy doing," Williams said.
By recruiting new muscle fibers and increasing the body’s ability to use fuel, interval training could potentially lower the risk of metabolic syndrome.
Interval training does amount to hard work, but the sessions can be short. Best of all, a workout that combines tortoise and hare leaves little time for boredom.
Work Out Now, Ache Later: How Your Muscles Pay You Back
By Vicky Lowry : New York Times. November 16, 2004
Active people know the feeling all too well: a stiff and achy sensation in the muscles that sneaks up on the body 24 hours or more after, say, a hard run, a challenging weight lifting session or the first day back on the ski slopes.
Sports scientists call it delayed onset of muscle soreness. Athletes call it a nuisance because even simple movements like walking down stairs can be an ordeal. If the soreness is severe enough, it can hamper the next workout or even ruin a ski vacation.
Because of the delay, some people may not even realize that the aches and pains were caused by an activity - gardening, for example, or hammering nails - engaged in days before.
"I've had patients call me up who think they have a virus," said Dr. Gary Wadler, a professor at the New York University School of Medicine and a specialist in sports medicine.
The culprit for delayed muscle soreness is not, as some people used to think, the buildup of lactic acid, a byproduct of exercise that dissipates from the muscle tissues within an hour. That kind of soreness is considered acute. As soon as someone stops exercising, or shortly afterward, the burn goes away.
"It's not the key bad guy," said Dr. Michael Saunders, director of the Human Performance Laboratory at James Madison University in Harrisonburg, Va.
No one knows for sure exactly what does cause muscle soreness. But many scientists now think that the delayed pain is caused by microscopic tears in the muscles when a certain exercise or activity is new or novel. These tiny tears eventually produce inflammation, and corresponding pain, 24 to 36 hours later.
"White blood cells start to repair the damaged muscle after about 12 to 24 hours and they release a number of chemicals which are likely to be involved in the generation of local muscle pain," said Dr. Mark Tarnopolsky, a specialist in neuromuscular disorders at the McMaster University Medical Center in Hamilton, Ontario. "You see damage at the microscopic level immediately after exercise, yet the soreness is usually delayed for about 24 hours and peaks at 48 hours."
The good news is that as these little tears repair themselves, they prepare the muscles to handle the same type of exercise better the next time.
"The muscle gets more resilient, meaning the next time you do that same exercise you won't get damaged as much," said Dr. Priscilla Clarkson, a professor of exercise science at the University of Massachusetts and a leading researcher on muscle soreness. "That doesn't mean you are stronger, or mean you can lift more weight. It just means your muscle fibers are likely stronger so they won't tear as easily. Over time they'll build up and become a stronger fiber to lift more weight."
Performing certain exercises can almost guarantee delayed soreness: running, hiking or skiing downhill, for example, and lowering weights - what weight lifters refer to as "negatives." In these downhill or downward motions, called eccentric muscle actions, the muscle fibers have to lengthen and then contract, "like putting on the brakes," Dr. Clarkson explained. "It's that lengthening-contraction that puts the most strain on the fiber and does the most damage."
Of the 600 or so muscles in the human body, about 400 of them are skeletal. The largest of these are the muscles most susceptible to delayed soreness, Dr. Wadler said.
Severe muscle pain that lasts for many days can be a sign of rhabdomyolysis, a disorder that occurs when too much of the muscle protein myoglobin leaks from the muscle cells into the bloodstream, possibly damaging the kidneys.
Dark urine, indicating the presence of myoglobin, can be a symptom of rhabdomyolysis, which in very rare cases can lead to renal failure.
Running marathons and participating in other endurance events can cause rhabdomyolysis, said Dr. William O. Roberts, president of the American College of Sports Medicine. Other risk factors include being unfit or dehydrated and exercising in high temperatures.
"It's one of the reasons why you want to stay well hydrated if you are going to work your muscles hard," Dr. Roberts said. "Drink enough so that you have good urine output to clear these waste products." In most cases, though, delayed muscle soreness is not serious, and the soreness fades after a day or two of rest. Weight lifters typically work out the lower body one day and the upper body the next to give fatigued muscles a chance to recover. And conditioned athletes, like cyclists and runners, often alternate between easy and hard days of exercise. "Stress-adapt, stress-adapt so you can handle more and more exercise," said Dr. Tarnopolsky. "That's what an athlete strives for."
The results for other strategies for avoiding or recovering more quickly from muscle soreness are mixed. Many active people reach for nonsteroidal anti-inflammatory drugs like Advil or Aleve. While some data suggest that the drugs may work to prevent soreness or alleviate it once it sets in, the degree of reduction in soreness is small, Dr. Clarkson said.
Rarely, doctors prescribe the painkillers known as COX-2 inhibitors for short-term muscle soreness. But the drugs, which include Celebrex and Bextra, are more commonly used to treat arthritis.
And all cox-2 inhibitors are under increased scrutiny, after Vioxx was pulled from the market in September. Merck withdrew it after studies found it increased the risk of heart attacks and stroke.
Stretching does not prevent muscle soreness, researchers have found, and massage does little to improve recovery after eccentric muscle use, according to a study published in September in The American Journal of Sports Medicine. In the study, researchers in Stockholm found that after participants performed leg exercises to exhaustion, massage treatment did not affect the level or duration of pain, loss of strength or muscle function.
Consuming protein, however, may help. In a report published in the July issue of the journal Medicine & Science in Sports & Exercise, scientists found that trained cyclists who consumed a carbohydrate and protein beverage during and immediately after a ride, were able to ride 29 percent longer during the first ride, and 40 percent longer in a second session than those consuming carbohydrates alone.
"Our findings suggest that the protein-carbohydrate mix enhanced muscle performance and recovery in the later rides," said Dr. Saunders of James Madison, the study's lead author.
But further research is necessary. The results of the study may have been influenced by a higher caloric content in the carbohydrate-protein beverage.
"There is some evidence that consuming protein and carbohydrates in the immediate period after exercise may decrease subsequent muscle damage, but that research is in its infancy," said Dr. Tarnopolsky. "What has been fairly well established is that eating food in the postexercise period is better than starving.
"The take-home message is if you are training in the evening don't go to bed on an empty stomach. And if you work out in the morning, eat breakfast afterward or make darn sure to take a snack to work."
A practical tactic is to try to limit muscle soreness before it takes hold. For that, you need to train the body to get used to downhill or downward motions.
"Gradually run or walk down hills more if you are planning to participate in a downhill event, or take an elevator up to the top of a tall building and walk or run down the stairs," Dr. Roberts recommended.
Hikers should consider using adjustable poles, which distribute some of the stress on the legs, transferring it to the upper body, when descending steep grades. "I put hiking poles into the hands of every one of my clients and tell them that if they don't like them I'll carry them," said Nate Goldberg, who routinely guides hikes up 14,000-foot peaks in the Sawatch Mountains of Colorado as director of the Beaver Creek Hiking Center. "Very rarely do I get a set of poles back."
Seasoned athletes, it turns out, are no more immune to delayed onset of muscle soreness than neophyte exercisers. "If I asked Lance Armstrong to run down 10 flights of stairs, he'd be very sore," Dr. Clarkson said. "It's all about sport specificity."
Can Exercise Kill?
The answer: Yes, and probably more often than you think
By Kevin Helliker : Wall Street Journal : October 11, 2004
· In the space of seven months in 2002, three physicians at Johns Hopkins Hospital in Baltimore suffered sudden cardiac death while exercising. Two were running, the other working out in the hospital's fitness center. All three had paid close attention to diet and exercised regularly. The oldest was 51.
This unlikely string of deaths brought tremendous local attention to a topic that medicine typically doesn't emphasize -- for good reason. Exercise, after all, prolongs more lives than it cuts short. And in a nation that is largely sedentary, people need no extra excuse not to exercise.
Yet a growing number of physicians believe that publicizing the risks of exercise could potentially save a significant number of lives. Johns Hopkins cardiologist Nancy Strahan, for one, is now advising her middle-aged patients to stay away from jogging until they've undergone an exam to determine their risks.
"Present research reveals that vigorous exercise is responsible for triggering up to 17%" of sudden cardiac deaths in the U.S., says a recent article in the American Medical Athletic Association Journal. This means that vigorous exercise is triggering tens of thousands of U.S. deaths a year.
Impact on Immune System
What's more, sudden death isn't the only risk. Evidence is mounting that extreme exercise -- marathons, triathlons and the like -- may be detrimental to the immune system and long-term health. "Exercising to excess can harm our health," cautions Kenneth Cooper, the physician credited with founding the aerobics movement back in the 1960s.
All of this, of course, runs counter to conventional wisdom, which says that exercise is a virtue, and that you can't get too much of a virtue. Indeed, pretty much as soon as a thirtysomething slips on his first pair of running shoes he is challenged by an acquaintance or athletic-store poster to run a marathon. But exercise more accurately may be perceived as a medical therapy, and doctors are generally very cautious about the dosages they prescribe for medical therapies. Nobody would recommend quadrupling the dose of a drug that had proved to be effective.
So, how much is too much? It depends, of course, on the person.
The risk of sudden cardiac death during exercise would be reduced if people -- especially those older than 40 -- underwent various tests before starting a workout program. These tests include: an electrocardiogram, an electrical recording of the heart that can detect various abnormalities; an exercise stress test, during which physicians monitor the cardiovascular system's response during a treadmill workout; and an echocardiogram, an ultrasound scan that can spot a wide range of defects. Whether your insurance will pay for these tests depends on your age, health plan and how strongly your doctor recommends them.
Although these tests aren't guaranteed to find every cardiovascular booby trap that exercise can trip, they can identify a significant percentage of the conditions that cause sudden cardiac death-artery blockages, cardiac arrhythmias, aneurysms and more.
The risk of sudden death during exercise appears to rise as the duration of the workout grows. For instance, the risk of death during a marathon is about one in 50,000 finishers -- significantly higher than during shorter races or inactivity. One reason is that during long-distance runs the body sustains muscle injury, and it can react to this injury as if it were bleeding, by rendering blood more clottable, says Arthur Siegel, a Harvard University professor and chief of internal medicine at McLean Hospital in Belmont, Mass. In people with hidden blockage in their coronary arteries, this thickened blood can result in sudden cardiac death.
But that's not the only danger. Muscular injury can also set off a hormonal response that in turn triggers water intoxication, with acute brain swelling, says Dr. Siegel. This can be deadly for marathon runners who take too seriously the recommendation to drink lots of fluid. In recent years, young and healthy runners have died of hyponatremia -- essentially drinking too much fluid -- in several marathons, including those in Chicago and Boston.
"A half-million Americans a year are going out to run marathons," says Dr. Siegel. "They incur a dose of exercise that is enough to cause muscle injury that could, under certain circumstances, have grave consequences."
Having run 20 marathons himself, Dr. Siegel calls himself an advocate for safe participation. Avoiding hyponatremia is mostly a matter of drinking only when thirsty, and this caution is especially important for slower runners.
As for sudden cardiac death, Dr. Siegel suggests that people at risk for cardiac disease perhaps should be cautious about pushing their heart rates too high. People with high risk factors "ought to be careful about keeping the intensity moderate," says Dr. Siegel. "Exercise at a level where they can be conversational." Should such people run marathons? Dr. Siegel advises: "Do the marathon training but skip the race."
An increasingly popular theory has it that death from extreme exercise may not come until years afterward. This theory first occurred to Dr. Cooper, founder of the Cooper Institute in Dallas, when he noticed what seemed like a higher-than-average rate of cancer and other disease among the fitness fanatics he knew.
'More Harm Than Good'?
Having now studied the matter for more than 20 years, he has concluded that especially long and intense bouts of exercise may be damaging to the immune system. It is only a theory, but it is at least partly based on medical studies such as one showing that marathoners suffer a high rate of cold and flu just before and after races.
"If you're exercising more than five hours a week [at a high intensity], there's a possibility that you may be doing more harm than good," Dr. Cooper says.
Nobody should feel compelled for health reasons to run marathons, do triathlons or otherwise aspire to become a fitness fanatic, says Dr. Cooper, adding that 30 minutes a day of moderate exercise such as walking is sufficient.
Of course, there are benefits to extreme exercise -- it provides enormous relief from stress and consumes a spectacular number of calories. For people committed to exercising fanatically, Dr. Cooper and others recommend diets heavy in antioxidants such as green vegetables, as well as supplements such as vitamins C and E. Such diets are believed to bolster the immune system.
Devotees of extreme exercise express confidence that any risks, including a possible increased vulnerability to cancer, are outweighed by benefits ranging from lowered blood pressure to heightened confidence. This explains why Frank Webbe, a professor of psychology at Florida Institute of Technology, has run 14 marathons.
"You run them because you can," says Dr. Webbe, a veteran officer of a group called Running Psychologists. Marathons, he says, are "part of my identity. It's a self definition. I'm one of the elite few. It's important to me."
Is marathoning too good a thing for your heart?
By Gretchen Reynolds : NY Times article : December 7, 2006
HE had not expected to spend his 60th birthday in a hospital cardiac unit. R. J. Turner, a commercial real estate broker from Frederick County, Va., had planned a robust celebration. “I was going to finish my 10th marathon,” Mr. Turner said, “which isn’t bad for a guy my age.”
But near the start of the Marine Corps Marathon on Oct. 29, Mr. Turner raised an arm to wave at bystanders, and “everything went black.” Collapsing violently, he gashed his head, chipped a tooth and bit a deep hole in his bottom lip.
Mr. Turner, who had passed a stress test a year before, had just had a heart attack.
This has been an unusual season for the cardiac health of marathoners. After years in which almost no deaths were attributed to heart attacks at this country’s major marathons, at least six runners have died in 2006.
Two police officers, one 53, the other 60, died of heart attacks at the Los Angeles Marathon in March. The hearts of three runners in their early 40s gave out during marathons in Chicago in October, San Francisco in July and the Twin Cities in October. And at the same marathon where Mr. Turner was felled, another man, 56, crumpled near the 17th mile, never to recover.
This year’s toll has sobered race directors and medical directors of marathons. But, as Rick Nealis, the director of the Marine Corps Marathon, said, “Statistically, maybe, it was inevitable.”
Race fields have grown. In 2005, 382,000 people completed a marathon in the United States, an increase of more than 80,000 since 2000, according to marathonguide.com. Meanwhile, the risk of dying from a heart attack during a marathon is about 1 in 50,000 runners, said Dr. Arthur Siegel, the director of internal medicine at McLean Hospital in Belmont, Mass., and an assistant professor of medicine at Harvard.
But some physicians, including Dr. Siegel, an author of more than two dozen studies of racers at the Boston Marathon, wonder if there is more to the deaths than mathematical inevitability: Does racing 26.2 miles put a heart at risk?
A new study by Dr. Siegel and colleagues at Massachusetts General Hospital and other institutions is at least suggestive. Sixty entrants from the 2004 and 2005 Boston Marathon were tested before and after the race. Each was given an echocardiogram to find abnormalities in heart rhythm and was checked for blood markers of cardiac problems — in particular for troponin, a protein found in cardiac muscle cells. If the heart is traumatized, troponin can show up in the blood. Its presence can determine whether there has been damage from a heart attack.
The runners (41 men, 19 women) had normal cardiac function before the marathon, with no signs of troponin in their blood. Twenty minutes after finishing, 60 percent of the group had elevated troponin levels, and 40 percent had levels high enough to indicate the destruction of heart muscle cells. Most also had noticeable changes in heart rhythms. Those who had run less than 35 miles a week leading up to the race had the highest troponin levels and the most pronounced changes in heart rhythm.
The findings, published in the Nov. 28 issue of Circulation, a journal of the American Heart Association, were a surprise, and not least to the runners. None had reported chest pains or shortness of breath at the finish. All had felt fine, Dr. Siegel said (to the extent one can feel fine after pounding through 26.2 miles).
Within days, the abnormalities disappeared. But something seemed to have happened in the race. “Their hearts appeared to have been stunned,” Dr. Siegel said.
“Although the evidence is not conclusive, it does look like the Boston study is showing some effect on cardiac muscle,” said Dr. Paul D. Thompson, 59, the director of cardiology at Hartford Hospital in Connecticut, and an author of an editorial that accompanied the study. “It’s far too early to draw any conclusions,” he added. “We’d be seeing lots more bodies piling up if there were real lingering long-term cardiac damage” caused by running marathons.
“Over all, the evidence is strongly in favor of the idea that endurance exercise is helpful in terms of cardiac health,” said Dr. Thompson, who has run more than 30 marathons.
But questions do remain. Another new study, this one out of the University of Duisburg-Essen in Germany, showed completely unexpected results in a group of experienced middle-aged male marathoners. In the study, which was presented in November at a meeting of the American Heart Association, the subjects, each of whom had completed at least five marathons, underwent an advanced type of heart screening called a spiral CT scan. Unlike echocardiograms or stress tests, spiral CTs show the level of calcium plaque buildup or atherosclerosis in the arteries.
More than a third of the runners had significant calcium deposits, suggesting they were at relatively high risk for a heart attack. Only 22 percent of a control group of nonrunners had a comparable buildup.
The researchers scrupulously avoided suggesting that marathoning had caused the men to develop heart disease. (After all, running may have kept them alive when they would otherwise have keeled over years earlier.) But neither did the authors rule out the possibility that in some baffling way distance running had contributed to the men’s arterial gunk.
What worries Dr. Siegel and some of his colleagues is that marathons present an opportunity for silent symptomless heart disease to introduce itself abruptly. The pulsing excitement, the adrenaline, the unpleasant process of “hitting the wall” may trigger physiological changes that loosen arterial plaques, precipitating a heart attack, Dr. Siegel said.
His advice to runners with any history of heart trouble is “train for the race, getting the cardiac benefits of endurance exercise,” then watch the event on television.
The risk of going into cardiac arrest as a spectator, he said, is only about one in a million. (The applicable studies of spectators involved Super Bowl fans.)
Anyone considering joining the ranks of marathoners should undergo a full medical screening, with a visit to a cardiologist for those over 40, Dr. Siegel said. Spiral CT scans are desirable (the cost can range from $250 to $850) and are covered by insurance if recommended by a physician.
Those with a family history of cardiac problems should be especially cautious. “You can’t outrun your genes,” Dr. Siegel said, a reality that marathon medical experts call the Jim Fixx effect, after the author of “The Complete Book of Running,” who died of a heart attack in 1984 at 52. His father had also died young.
Still, the majority of cardiologists remain avid fans of marathons. “It is an extraordinary event,” said Dr. Frederick C. Lough, the director of cardiac surgery at George Washington University in Washington. “But you have to respect that distance. It’s not something everyone necessarily should attempt.”
Dr. Lough, 57, was less than a block behind Mr. Turner when the older man collapsed. He interrupted his own race to help revive Mr. Turner and accompany him to the hospital, before completing the marathon. “It was a vivid reminder that running does not make anyone immune to heart disease,” Dr. Lough said.
Experts familiar with the new cardiac studies of marathoners urge caution and perspective. The numbers of people studied were small, the findings unexplained, and results have not yet been replicated.
Don’t use the studies, in other words, to justify parking yourself smugly on the couch. “There’s not yet in my opinion cause for alarm,” Dr. Thompson said. “I would still tell people, run.”
His words doubtless will cheer Mr. Turner. “You know the worst thing about almost dying?” he said. “That I didn’t finish.” After having had a stent installed in his heart to open an artery that was about 98 percent blocked, he’s now walking a mile a day and planning his comeback. “I want to get that 10th marathon in,” he said.
But not before he gets a full medical screening, including a spiral CT scan.
·
Fitness: It’s O.K. to Run Hurt
By Gina Kolata ; NY Times article : January 11, 2007
JUST before the end of last year, a prominent orthopedic surgeon was stretching to lift a heavy box and twisted his back. The pain was agonizing. He could not sit, and when he lay down he could barely get up.
So the surgeon, Dr. James Weinstein of Dartmouth College, decided to go out for a run.
“I took an anti-inflammatory, iced up, and off I went,” Dr. Weinstein recalled. When he returned, he said, he felt “pretty good.”
It sounds almost like heresy. The usual advice in treating injuries is to rest until the pain goes away. But Dr. Weinstein and a number of leading sports medicine specialists say that is outdated and counterproductive. In fact, Dr. Weinstein says, when active people consult him, he usually tells them to keep exercising.
The idea, these orthopedists and exercise specialists say, is to use common sense. If you’ve got tendinitis or sprained a muscle or tendon by doing too much, don’t go right back to exercising at the same level.
The specific advice can differ from specialist to specialist. Some, like Dr. Weinstein, say most people can continue with the sport they love although they may need to cut back a bit, running shorter distances or going more slowly. Others say to cross-train at least some of the time and others say the safest thing to do is to cross-train all the time until the pain is gone. You might end up cycling instead of running, or swimming instead of playing tennis. But unless it’s something as serious as a broken bone or a ripped ligament or muscle, stopping altogether may be the worst thing to do.
“We want to keep you moving,” said Dr. William Roberts, a sports medicine specialist at the University of Minnesota and a past president of the American College of Sports Medicine. “Injured tissue heals better if it’s under some sort of stress.”
He and others acknowledge that the advice to keep moving may come as a surprise and that some doctors feel uncomfortable giving it, worried that their patients will do too much, make things worse and then blame their doctor.
“I’m not convinced this is part of every doctor’s training or that everyone is ready to make it part of mainstream medicine,” Dr. Roberts said. “You have to work with athletes a while to figure out how to do it and how to do it well.”
“The easy way out is to say, ‘Don’t exercise,’ ” said Dr. Richard Steadman, an orthopedic surgeon in Vail, Colo., and founder of the Steadman Hawkins Research Foundation, which studies the origins and treatment of sports injuries. That advice, he added, “is safe and you probably will have healing over time.” But, he said, “if the injury is not severe, resting it will probably prolong recovery.”
Medical researchers say that they only gradually realized the importance of exercising when injured. A few decades ago, Dr. Mininder Kocher, a sports medicine specialist and orthopedic surgeon at Children’s Hospital Boston, said doctors were so intent on forcing hurt athletes to rest that they would put injured knees or elbows or limbs in a cast for two to three months.
When the cast finally came off, the patient’s limb would be stiff, the muscles atrophied. “It would take six months of therapy to get strength and motion back,” Dr. Kocher said.
At the same time, in a parallel path, researchers were learning that painful conditions that are essentially inflammation — arthritis and chronic lower back pain — actually improve when patients keep moving.
Now some researchers, like Dr. Freddie Fu, a sports medicine expert and chairman of the orthopedic surgery department at the University of Pittsburgh Medical Center, and a colleague, James H-C. Wang, are studying minor injuries at the molecular level.
Their focus is on tendinitis — the inflamed tendons that are the bane of many exercisers and that affect 15 to 20 percent of all Americans at any given time. The symptoms are all too familiar — pain, swelling and soreness. To study the injury process, Dr. Wang grows human tendons in the laboratory, stretching them repeatedly. In separate experiments, he has mice run on treadmills until their tendons begin to show the tiny microscopic tears that occur in the early stages of tendinitis.
So far, Dr. Wang reports, he and Dr. Fu learned some important lessons: First, forceful stretching of tendons elicits the production of molecules that are involved in inflammation. But small repeated stretching of tendons that are already inflamed leads to the production of molecules that heal inflammation. That suggests moderate exercise can actually speed healing.
And now, their preliminary results suggest that the usual treatment for tendinitis — taking drugs like aspirin or ibuprofen — can help reduce inflammation when the injury begins. But after inflammation is under way, they can make matters worse.
But medical experts caution that people have to be careful if they try to exercise when they are injured.
Some, like Dr. Fu, who is himself a cyclist, Dr. Roberts, and Dr. Steadman say the first priority is to see a doctor and get an accurate diagnosis in order to rule out a serious injury.
Others, like Dr. Weinstein, say that such an injury, a broken bone or a torn Achilles tendon, for example, has symptoms so severe that it is obvious something is really wrong.
“If you had inflammation and swelling that was very tender to the touch, you would know,” Dr. Weinstein said. And if you tried to exercise, it would hurt so much that you just could not do it.
Dr. Weinstein’s advice for injured patients is among the boldest — he said it’s based on his basic research and his own experience with sports injuries, like knee pain and tendinitis of the Achilles and hamstring. Before exercise, he said, take one anti-inflammatory pill, like an aspirin. Ice the area for 20 minutes. Then start your usual exercise, the one that resulted in your injury, possibly reducing the intensity or time you would have spent. When you finish, ice the injured area again.
The advice involving an anti-inflammatory pill, Dr. Weinstein said, is based on something surgeons know — in most cases, a single anti-inflammatory pill before surgery results in less pain and swelling afterward. It also is consistent with Dr. Wang’s research because, at least in theory, it should forestall new inflammation from the exercise that is about to occur.
The icing is to constrict blood vessels before and after exercise, thereby preventing some of the inflammatory white blood cells from reaching the injured tissue.
Dr. Steadman, who works with injured athletes in his clinic, does not advise trying to go back to your old exercise on your own until the pain is completely gone. Play it safe, he said, and cross-train.
But others, like Dr. Fu and Dr. Kocher, are more inclined to suggest trying your old sport. Both also tell injured patients to ice before and after exercising. Dr. Kocher said he sometimes advises taking an anti-inflammatory pill, but worries about masking pain so much that patients injure themselves even more by overdoing the exercise.
His rule of thumb, Dr. Kocher said, is that if the pain is no worse after exercising than it is when the person simply walks, then the exercise “makes a lot of sense.”
It also helps patients psychologically, he added. “If you take athletes or active people out, they get depressed, they get wacky,” Dr. Kocher explained.
Noah Hano knows all about that.
Mr. Hano, 34, a commercial real estate broker in Boston, was competing in marathons and triathlons. Then he developed severe sciatica, whose pain is a direct result of inflammation. He tried physical therapy, he tried acupuncture, he tried massage therapy, but nothing quelled the “nagging, terrible pain” down his leg, he said.
He stopped exercising, but the pain persisted.
“I started getting desperate,” Mr. Hano said. His father, who lives in the same town as Dr. Weinstein, suggested that Mr. Hano call the Dartmouth orthopedist. Dr. Weinstein told him to continue to exercise. Mr. Hano could not wait to get started. “I drove to the gym and ran on the treadmill,” he said. “When I woke up the next morning, I went for a swim and rode my bike. It hurt, but when the doctor told me I wasn’t going to be paralyzed, it made it a lot easier.”
Dr. Weinstein said that Mr. Hano’s problem was a huge, bulging disk, a herniation so severe that most doctors would say he should stop running immediately. Dr. Weinstein, though, thought exercise would help Mr. Hano heal. His treatment was a single injection of cortisone into the inflamed area around his disk. The sciatica gradually went away. And Mr. Hano continues to run.
“I had faith that I was going to be able to work through it,” Mr. Hano said. “I don’t want to not do what I like just because I’m in pain.”
Daily supplements
By Gretchen Reynolds : NY Times article : March 4, 2007
It’s no surprise that athletes like their dietary supplements. By conservative estimates, they spend nearly $4 billion annually on pills, powders and other sports-nutrition products in the hope that they’ll improve health and increase performance. New Orleans Saints center Jeff Faine recently told a reporter that he takes about 65 pills a day; for the sake of time management, he has taught himself to swallow as many as 17 at a time. This daily gorging pales next to that of Bill Romanowski, the former linebacker. In his 2005 autobiography, “Romo: My Life on the Edge,” Romanowski writes that he kept a tackle box filled with some 500 pills and would take handfuls a day, all washed down with protein shakes. He also famously admits to taking vials of THG, an anabolic steroid, but most of what he consumed were legal supplements available at any Walgreens or GNC store.
· Such supplements are not necessarily benign. In 2003, Baltimore Orioles pitcher Steve Bechler died, in part, from a reaction to ephedrine, a wildly popular supplement used to increase energy and metabolism. Ephedrine, a stimulant derived from the ephedra plant, can elevate heart rate and blood pressure, in some cases fatally. It’s now illegal to market ephedrine as a dietary supplement, though it’s still widely available, often as a decongestant or a cold remedy. Sales are brisk.
· Which underscores the disturbing truth about supplements: science and common sense often have less effect on their use than hope, hype and word of mouth. “A lot of the information about supplements is generated by the manufacturers or by personal testimonials,” says Kathleen Laquale, a leading nutritionist and an associate professor of athletic training at Bridgewater State College in Massachusetts. “Someone at the machine next to you in the gym says, ‘You’ve got to try this.’ ”
· That person could be right. Some supplements do what they promise. But the vast majority are ineffective — hard news for people (like me) who load up on vitamins and other pills and powders in the belief that they must be doing something. So how to separate the dross from the goods? Aside from the obvious — don’t take a supplement you haven’t thoroughly researched — it’s a matter of trial and error. What works for others might not work for you. Also bear in mind that positive results may have more to do with what’s going on in your mind than in your body. Try a high-profile supplement, some of the most popular of which are discussed here, and chances are you’ll swear it works, even if, strictly speaking, it doesn’t. The placebo effect, Laquale says, “is still an effect.”
Vitamins and Minerals: Way Too Much of a Good Thing
Unless you’re on an outré diet (grapefruit, cabbage soup, even Atkins), you’re probably getting enough daily nutrients without help from pills. “Most Americans easily get 100 percent of the vitamins and minerals they need from their food,” says Ellen Coleman, a sports dietician who consults for the Los Angeles Lakers and Angels.
It’s often presumed, however, that athletes need more than their three balanced meals a day. Heavy exertion increases the body’s use of oxygen and subsequently produces more free radicals: unstable atoms and molecules known to be harmful to cells. In theory, athletes should benefit from extra doses of antioxidants like vitamins C and E, beta carotene and coenzyme Q10, which reduce free radicals.
But research has produced mixed results. Several recent studies of animals suggested that large single doses of antioxidants (1,000 I.U. of vitamin E, say, instead of 100 I.U.) actually increased signs of oxidative damage; other studies have suggested that antioxidants might help speed muscle recovery, particularly for older athletes. To further the confusion, researchers have recently speculated that those who exercise less vigorously could possibly benefit more from antioxidant supplements than could elite athletes, whose bodies, the thinking now goes, might be better equipped to combat oxidative stress.
Athletes also tend to overdo the B-complex vitamins. Because B vitamins are essential for turning carbohydrates, fats and proteins into energy, many vitamins contain — and trumpet on their labels — mega-doses of the stuff. But “there’s not much evidence that extra doses of B vitamins give you better athletic performance or anything else,” Laquale says — besides a lighter wallet.
If you still can’t bear the thought of parting with your vitamins, limit yourself to a one-a-day multivitamin. “It’s hard to overdose on any one nutrient that way,” says Alicia Kendig, a sports dietician with Carmichael Training Systems in Colorado Springs, “and it gives you that little bit of extra insurance that you’re getting all the nutrients you need.”
Creatine: Speed, Strength and Some Minor Gastric Upset
Creatine, an amino acid compound stored in muscle tissue, is the top-selling sports supplement in the country. Available in powdered form, it aids the production of phosphocreatine (PCr), an important fuel used during short, intense exercise.
This is one supplement that actually seems to work. “There’s solid research that creatine helps to increase muscle mass and strength,” Coleman says. One recent study of male United S tates Army soldiers found that those taking creatine could do 14 percent more bench press repetitions than those taking a placebo. And a 2002 study conducted by Australian researchers showed that elite female soccer players who took the supplement were faster in a series of sprints than those on a placebo.
But creatine’s benefits are limited to activities that demand strength or short bursts of speed. It won’t do much for marathoners or other distance athletes. It’s not gentle on the system, either. Creatine pulls water into muscles, and in the process can dehydrate the rest of the body. Studies done in the late 1990s suggested that there were links between the supplement and muscle cramping and diarrhea, but those side effects were found at doses higher than what is generally recommended today. Coleman says five grams a day should get you the benefits without too much . . . distress.
DHEA: Increased Productivity at the Testosterone Factory?
Dehydroepiandrosterone, or DHEA, is a hormone produced naturally in human adrenal glands. Without it, the body can’t make testosterone or estrogen. Because of this link to testosterone, many athletes take DHEA capsules in the hope of building more muscle.
Studies conducted in the 1990s showed that rats and mice developed stronger bones, muscles and immune systems when given DHEA. Rodents, however, produce little DHEA naturally, so some researchers speculated that the supplement merely acted as a temporary jolt to their systems. Although a few small studies suggested that some elderly people with low levels of DHEA benefited from taking the supplements, the overall results were equivocal.
Then last October, in the , New England Journal of Medicine researchers from the Mayo Clinic published the results of a two-year, double-blind study on the efficacy of DHEA. The study found no beneficial effects. A 75-milligram daily dose for men did increase blood levels of DHEA but didn’t increase muscle strength or oxygen consumption. Neither did it decrease body fat. DHEA had no “physiologically relevant beneficial effects,” the authors concluded.
Undeterred, the Council for Responsible Nutrition, a trade group for the supplement industry, released a statement saying that the Mayo study confirmed “the safety of relatively high-dose DHEA.” It didn’t work, but it didn’t kill anyone, either.
It’s this kind of cheery obfuscation that keeps the supplement industry humming. “The amount of deliberate misinformation out there is amazing,” Laquale says. “It would be funny if it weren’t so disturbing.”
Because the Food and Drug Administration doesn’t closely regulate the nutritional supplement business — a 1994 law exempted supplements from strict oversight — the claims made by manufacturers tend to be extravagant. (“Instantly Triggers Extreme Muscle Expansion!”) The fine print adds that these statements have not been evaluated by the F.D.A. “But most people don’t read that far,” Coleman says.
Where, then, can you look for reliable, unbiased information? One place to start is ConsumerLab.com, an independent research organization that tests supplements. A yearly subscription to the site, which posts all of the lab’s product reports, costs $27.
In some instances, supplements tested by ConsumerLab have been found to contain ingredients not printed on their labels. A recent test of weight-loss supplements found that some were contaminated with lead. More often, though, the lab discovers what’s not in the supplement. ConsumerLab’s creatine study, for example, revealed products that contained little or no creatine at all. “The labels of supplements can be misleading,” says Tod Cooperman, a medical doctor who specializes in pharmaceuticals and is ConsumerLab’s president. “You should always be skeptical.”
One abiding fact about supplements is that their allure waxes and ebbs. The newest “it” supplement is resveratrol, a substance found in the skin of red grapes that was recently shown to protect against weight gain in rodents and to almost double the animals’ endurance on a treadmill. Since the results of this research were announced last year, companies have been scrambling to produce resveratrol formulations. Dozens are now available.
Studies have yet to be conducted to determine whether resveratrol improves performance in humans. Until then, it might be easier just to swallow your vitamins with a glass of Shiraz.
Exercise Overview
Physical activity is any activity that causes your body to work harder than normal. The actual amount of physical activity you need depends on your fitness goals, whether you are trying to lose weight, and how fit you are right now.
Physical activity can help you:
- Burn calories and reduce body fat
- Reduce your appetite
- Keep your current weight and control it
The number of calories burned during physical activity depends on:
- The amount of time you spend on physical activity: For example, walking for 45 minutes will burn more calories than walking for 20 minutes.
- Your body weight: For example, a 250-pound person will burn more calories walking for 30 minutes than a 185-pound person.
- Pace: For example, walking 3 miles per hour will burn more calories than walking 1.5 miles per hour.
Your basal metabolic rate (BMR) is the number of calories your body uses when it is at rest. BMR accounts for most of your calorie use. Your basal metabolic rate is based on things your body always does such as breathing, breaking down food, and keeping your heart and brain working. Your age, sex, body weight, and level of physical activity affect the basal metabolic rate. Basal metabolic rate increases with the amount of muscle tissue you have, and it reduces with age.
Along with burning more calories, physical activity increases the BMR, and the BMR can remain increased after 30 minutes of moderate physical activity. For many people, the basal metabolic rate can be increased for approximately 48 hours after the activity. This means, for example, that after the physical activity, when a person is sitting and watching television, the body is using more calories than usual.
EFFECT ON APPETITE
Physical activity at a moderate rate does not increase the appetite. In some situations, the appetite will actually decrease. Research shows that the decrease in appetite after physical activity is greater in individuals who are obese than in individuals who are at their right body weight.
LOSS OF BODY FAT
When losing weight just by taking in less calories, a person loses a quarter of his or her lean body mass, and three quarters of his or her body fat. Combining calorie reduction with physical activity can result in loss of 98% of body fat. Weight loss that is reached with a combination of calorie reduction and physical activity is more effective. For keeping a desirable body weight, a maintenance level of calories along with physical activity is recommended. This helps to preserve lean body mass and muscle tone.
RECOMMENDATIONS
For losing or maintaining weight:
- Try to do some form of physical activity at least three times a week. Increasing it to four to five times a week is even more helpful. Spread out the physical activity through the week rather than doing it on three or four consecutive days, to reduce the risk of injuries.
- The target heart rate during physical activity should be 60% to 90% of the maximum heart rate.
- 220(beats per minute) minus age = maximum heart rate.
- Maximum heart rate multiplied by the intensity level = target heart rate.
- 220 - 50 = 170 (maximum heart rate)
- 170 X 60% = 102 (target heart rate)
Physical activity at 60 to 70% of the maximum heart rate can be continued safely for a long period of time. If an exercise is too hard, conversation cannot be carried on during the physical activity (the person is out of breath).
According to the American College of Sports Medicine, physical activity of less than 2 times a week at less than 60% of the maximum heart rate, and for less than 10 minutes per day, does not help in developing and maintaining fitness. If physical activity is stopped, the fitness benefits are completely lost. Within 2 to 3 weeks the level of fitness is reduced, and within 3 to 8 months it is completely lost, and the person has to restart again.
Twenty minutes of continuous aerobic activity 3 days per week is recommended for weight loss. Examples of physical activity that are considered aerobic are: walking, running, jogging, hiking, swimming, bike riding, rowing, cross country skiing, and jumping rope.
BENEFITS
Physical activity contributes to health by reducing the heart rate, decreasing the risk for cardiovascular disease, and reducing the amount of bone loss that is associated with age and osteoporosis. Physical activity also helps the body use calories better, thereby helping with weight loss and weight maintenance. It can increase basal metabolic rate, reduces appetite, and help in the reduction of body fat.
SIDE EFFECTS
Physical activity should be done at a rate that is right for the person. An evaluation by an exercise physiologist is helpful, in order to to avoid injuries. Injuries can occur if physical activity is started without much consideration as to the type or length of the activity, and the physical condition of the person.
Does Exercise Really Keep Us Healthy?
By Gina Kolata : NY Times Article : January 8, 2008
Exercise has long been touted as the panacea for everything that ails you. For better health, simply walk for 20 or 30 minutes a day, boosters say — and you don’t even have to do it all at once. Count a few minutes here and a few there, and just add them up. Or wear a pedometer and keep track of your steps. However you manage it, you will lose weight, get your blood pressure under control and reduce your risk of osteoporosis.
If only it were so simple. While exercise has undeniable benefits, many, if not most, of its powers have been oversold. Sure, it can be fun. It can make you feel energized. And it may lift your mood. But before you turn to a fitness program as the solution to your particular health or weight concern, consider what science has found.
Moderate exercise, such as walking, can reduce the risk of diabetes in obese and sedentary people whose blood sugar is starting to rise. That outcome was shown in a large federal study in which participants were randomly assigned either to an exercise and diet program, to take a diabetes drug or to serve as controls. Despite trying hard, those who dieted and worked out lost very little weight. But they did manage to maintain a regular walking program, and fewer of them went on to develop diabetes.
Exercise also may reduce the risk of heart disease, though the evidence is surprisingly mixed. There seems to be a threshold effect: Most of the heart protection appears to be realized by people who go from being sedentary to being moderately active, usually by walking regularly. More intense exercise has been shown to provide only slightly greater benefits. Yet the data from several large studies have not always been clear, because those who exercise tend to be very different from those who do not.
Active people are much less likely to smoke; they’re thinner and they eat differently than their sedentary peers. They also tend to be more educated, and education is one of the strongest predictors of good health in general and a longer life. As a result, it is impossible to know with confidence whether exercise prevents heart disease or whether people who are less likely to get heart disease are also more likely to be exercising.
Scientists have much the same problem evaluating exercise and cancer. The same sort of studies that were done for heart disease find that people who exercised had lower rates of colon and breast cancer. But whether that result is cause or effect is not well established.
Exercise is often said to stave off osteoporosis. Yet even weight-bearing activities like walking, running or lifting weights has not been shown to have that effect. Still, in rigorous studies in which elderly people were randomly assigned either to exercise or maintain their normal routine, the exercisers were less likely to fall, perhaps because they got stronger or developed better balance. Since falls can lead to fractures in people with osteoporosis, exercise may prevent broken bones — but only indirectly.
And what about weight loss? Lifting weights builds muscles but will not make you burn more calories. The muscle you gain is minuscule compared with the total amount of skeletal muscle in the body. And muscle has a very low metabolic rate when it’s at rest. (You can’t flex your biceps all the time.)
Jack Wilmore, an exercise physiologist at Texas A & M University, calculated that the average amount of muscle that men gained after a serious 12-week weight-lifting program was 2 kilograms, or 4.4 pounds. That added muscle would increase the metabolic rate by only 24 calories a day.
Exercise alone, in the absence of weight loss, has not been shown to reduce blood pressure. Nor does it make much difference in cholesterol levels. Weight loss can lower blood pressure and cholesterol levels, but if you want to lose weight, you have to diet as well as exercise. Exercise alone has not been shown to bring sustained weight loss.Just ask Steven Blair, an exercise researcher at the University of South Carolina. He runs every day and even runs marathons. But, he adds, “I was short, fat and bald when I started running, and I’m still short, fat and bald. Weight control is difficult for me. I fight the losing battle.”
The difficulty, Dr. Blair says, is that it’s much easier to eat 1,000 calories than to burn off 1,000 calories with exercise. As he relates, “An old football coach used to say, ‘I have all my assistants running five miles a day, but they eat 10 miles a day.’”
Preserving a Fundamental Sense: Balance
By Jane E. Brody : NY Times Article : January 8, 2008
Scott McCredie is a Seattle-based health and science writer who says he “discovered” what he calls “the lost sense” of balance after he watched in horror as his 67-year-old father tumbled off a boulder and disappeared from sight during a hike in the Cascades.
Though his father hurt little more than his pride, Mr. McCredie became intrigued by what might have caused this experienced hiker, an athletic and graceful man, to lose his balance suddenly. His resulting science-and-history-based exploration led to a book, “Balance: In Search of the Lost Sense,” published last June by Little, Brown.
Noting that each year one in three Americans 65 and older falls, and that falls and their sometimes disastrous medical consequences are becoming more common as the population ages, Mr. McCredie wonders why balance is not talked about in fitness circles as often as strength training, aerobics and stretching. He learned that the sense of balance begins to degrade in one’s 20s and that it is downhill — literally and figuratively — from there unless steps are taken to preserve or restore this delicate and critically important ability to maintain equilibrium.
Vertigo, which can be caused by inner ear infections, low blood pressure, brain injuries, certain medications and some chronic diseases, is loss of balance in the extreme. Anyone who has experienced it — even if just from twirling in a circle — knows how disorienting and dangerous it can be. Really, without a sense of balance, just about everything else in life can become an insurmountable obstacle.
One normal consequence of aging is a steady decline in the three main sensory contributors to good balance — vision, proprioceptors on the bottoms of the feet that communicate position information to the brain, and the tiny hairs in the semicircular canals of the inner ear that relay gravity and motion information to the brain. Add to that the loss of muscle strength and flexibility that typically accompany aging and you have a fall waiting to happen.
But while certain declines with age are unavoidable, physical therapists, physiatrists and fitness experts have repeatedly proved that much of the sense of balance can be preserved and even restored through exercises that require no special equipment or training. These exercises are as simple as standing on one foot while brushing your teeth or walking heel-to-toe with one foot directly in front of the other.
Testing for Equilibrium
Marilyn Moffat and Carole B. Lewis, physical therapists in New York and Washington, respectively, agree with Mr. McCredie that “balance is an area of physical fitness that is often overlooked,” but they seek to correct that in their recent book “Age-Defying Fitness” (Peachtree Publishers). They define balance as “the ability of your body to maintain equilibrium when you stand, walk or perform any other daily activity” like putting on pants, walking on uneven ground or reaching for something on a shelf.
Dr. Moffat and Dr. Lewis suggest starting with a simple assessment of your current ability to maintain good balance. With a counter or sturdy furniture near enough to steady you if needed, perform this test:
1. Stand straight, wearing flat, closed shoes, with your arms folded across your chest. Raise one leg, bending the knee about 45 degrees, start a stopwatch and close your eyes.
2. Remain on one leg, stopping the watch immediately if you uncross your arms, tilt sideways more than 45 degrees, move the leg you are standing on or touch the raised leg to the floor.
3. Repeat this test with the other leg.
Now, compare your performance to the norms for various ages:
¶ 20 to 49 years old: 24 to 28 seconds.
¶ 50 to 59 years: 21 seconds.
¶ 60 to 69 years: 10 seconds.
¶ 70 to 79 years: 4 seconds.
¶ 80 and older: most cannot do it at all.
If you are wise, whatever your age, you will want to strive for the norm of those younger than 50. To increase stability and strengthen the legs, stand with feet shoulder-width apart and arms straight out in front. Lift one foot behind, bending the knee at 45 degrees. Hold that position for five seconds or longer, if possible.
Repeat this exercise five times. Then switch legs. As you improve, try one-leg stands with your eyes closed.
You can also incorporate one-leg stands into daily routines — while on the telephone, for example, brushing your teeth, waiting in line or for a bus, or cooking and washing dishes.
Exercises to Build a Motor Skill
“Remember, balance is a motor skill,” Dr. Moffat, professor of physical therapy at New York University, said in an interview. “To enhance it, you have to train your balance in the same way you would have to train your muscles for strength and your heart for aerobic capacity.”
Dr. Moffat pointed out that balance is twofold: static while standing still and dynamic when moving, as in walking and climbing stairs. Two main routes improve balance — exercises that increase the strength of the ankle, knee and hip muscles and exercises that improve the function of the vestibular system.
Like one-leg stands, many can be done as part of a daily routine. Dr. Moffat recommends starting with strength exercises and, as you improve, adding vestibular training by doing some of them with closed eyes.
Sit-to-stand exercises once or twice a day increase ankle, leg and hip strength and help the body adjust to changes in position without becoming dizzy after being sedentary for a long time. Sit straight in a firm chair (do not lean against the back) with arms crossed. Stand up straight and sit down again as quickly as you can without using your arms. Repeat the exercise three times and build to 10 repetitions.
Heel-to-toe tandem walking is another anytime exercise, resembling plank walking popular with young children. It is best done on a firm, uncarpeted floor. With stomach muscles tight and chin tucked in, place one foot in front of the other such that the heel of the front foot nearly touches the toe of the back foot. Walk 10 or more feet and repeat the exercise once or twice a day.
Also try walking on your toes and then walking on your heels to strengthen your ankles.
Another helpful exercise is sidestepping. Facing a wall, step sideways with one leg (bring the other foot to it) 10 times in each direction. After mastering that, try a dancelike maneuver that starts with sidestepping once to the right. Then cross the left leg behind, sidestep to the right again and cross the left leg in front. Repeat this 10 times. Then do it in the other direction.
In addition, the slow, continuous movements of tai chi, that popular Chinese exercise, have been shown in scientific studies to improve balance and reduce the risk of falls.
The Simple Push-Up as a sign of health and wellness
By Tara Parker-Pope : NY Times Article : March 11, 2008
As a symbol of health and wellness, nothing surpasses the simple push-up.
Practically everyone remembers the actor Jack Palance performing age-defying push-ups during his Oscar acceptance speech. More recently, Randy Pausch, the Carnegie Mellon professor whose last lecture became an Internet sensation, did push-ups to prove his fitness despite having pancreatic cancer.
"It takes strength to do them, and it takes endurance to do a lot of them," said Jack LaLanne, 93, the fitness pioneer who astounded television viewers in the 1950s with his fingertip push-ups. "It's a good indication of what kind of physical condition you're in."
The push-up is the ultimate barometer of fitness. It tests the whole body, engaging muscle groups in the arms, chest, abdomen, hips and legs. It requires the body to be taut like a plank with toes and palms on the floor. The act of lifting and lowering one's entire weight is taxing even for the very fit.
"You are just using your own body and your body's weight," said Steven G. Estes, a physical education professor and dean of the college of professional studies at Missouri Western State University. "If you're going to demonstrate any kind of physical strength and power, that's the easiest, simplest, fastest way to do it."
But many people simply can't do push-ups. Health and fitness experts, including the American College of Sports Medicine, have urged more focus on upper-body fitness. The aerobics movement has emphasized cardiovascular fitness but has also shifted attention from strength training exercises.
Moreover, as the nation gains weight, arms are buckling under the extra load of our own bodies. And as budgets shrink, public schools often do not offer physical education classes — and the calisthenics that were once a childhood staple.
In a 2001 study, researchers at East Carolina University administered push-up tests to about 70 students ages 10 to 13. Almost half the boys and three-quarters of the girls didn't pass.
Push-ups are important for older people, too. The ability to do them more than once and with proper form is an important indicator of the capacity to withstand the rigors of aging.
Researchers who study the biomechanics of aging, for instance, note that push-ups can provide the strength and muscle memory to reach out and break a fall. When people fall forward, they typically reach out to catch themselves, ending in a move that mimics the push-up. The hands hit the ground, the wrists and arms absorb much of the impact, and the elbows bend slightly to reduce the force.
In studies of falling, researchers have shown that the wrist alone is subjected to an impact force equal to about one body weight, says James Ashton-Miller, director of the biomechanics research laboratory at the University of Michigan.
"What so many people really need to do is develop enough strength so they can break a fall safely without hitting their head on the ground," Dr. Ashton-Miller said. "If you can't do a single push-up, it's going to be difficult to resist that kind of loading on your wrists in a fall."
And people who can't do a push-up may not be able to help themselves up if they do fall.
"To get up, you've got to have upper-body strength," said Peter M. McGinnis, professor of kinesiology at State University of New York College at Cortland who consults on pole-vaulting biomechanics for U.S.A. Track and Field, the national governing body for track.
Natural aging causes nerves to die off and muscles to weaken. People lose as much as 30 percent of their strength between 20 and 70. But regular exercise enlarges muscle fibers and can stave off the decline by increasing the strength of the muscle you have left.
Women are at a particular disadvantage because they start off with about 20 percent less muscle than men. Many women bend their knees to lower the amount of weight they must support. And while anybody can do a push-up, the exercise has typically been part of the male fitness culture. "It's sort of a gender-specific symbol of vitality," said R. Scott Kretchmar, a professor of exercise and sports science at Penn State. "I don't see women saying: 'I'm in good health. Watch me drop down and do some push-ups.' "
Based on national averages, a 40-year-old woman should be able to do 16 push-ups and a man the same age should be able to do 27. By the age of 60, those numbers drop to 17 for men and 6 for women. Those numbers are just slightly less than what is required of Army soldiers who are subjected to regular push-up tests.
If the floor-based push-up is too difficult, start by leaning against a countertop at a 45-degree angle and pressing up and down. Eventually move to stairs and then the floor.
Mr. LaLanne, who once set a world record by doing 1,000 push-ups in 23 minutes, still does push-ups as part of his daily workout. Now he balances his feet and each hand on three chairs.
"That way I can go way down, even lower than if I was on the floor," he said. "That's really tough."
April 12, 2010
Weighing the Evidence on Exercise
By GRETCHEN REYNOLDS
How exercise affects body weight is one of the more intriguing and vexing issues in physiology. Exercise burns calories, no one doubts that, and so it should, in theory, produce weight loss, a fact that has prompted countless people to undertake exercise programs to shed pounds. Without significantly changing their diets, few succeed. “Anecdotally, all of us have been cornered by people claiming to have spent hours each week walking, running, stair-stepping, etc., and are displeased with the results on the scale or in the mirror,” wrote Barry Braun, an associate professor of kinesiology at the University of Massachusetts at Amherst, in the American College of Sports Medicine’s February newsletter.
But a growing body of science suggests that exercise does have an important role in weight loss. That role, however, is different from what many people expect and probably wish. The newest science suggests that exercise alone will not make you thin, but it may determine whether you stay thin, if you can achieve that state. Until recently, the bodily mechanisms involved were mysterious. But scientists are slowly teasing out exercise’s impact on metabolism, appetite and body composition, though the consequences of exercise can vary. Women’s bodies, for instance, seem to react differently than men’s bodies to the metabolic effects of exercise. None of which is a reason to abandon exercise as a weight-loss tool. You just have to understand what exercise can and cannot do.
“In general, exercise by itself is pretty useless for weight loss,” says Eric Ravussin, a professor at the Pennington Biomedical Research Center in Baton Rouge, La., and an expert on weight loss. It’s especially useless because people often end up consuming more calories when they exercise. The mathematics of weight loss is, in fact, quite simple, involving only subtraction. “Take in fewer calories than you burn, put yourself in negative energy balance, lose weight,” says Braun, who has been studying exercise and weight loss for years. The deficit in calories can result from cutting back your food intake or from increasing your energy output — the amount of exercise you complete — or both. When researchers affiliated with the Pennington center had volunteers reduce their energy balance for a study last year by either cutting their calorie intakes by 25 percent or increasing their daily exercise by 12.5 percent and cutting their calories by 12.5 percent, everyone involved lost weight. They all lost about the same amount of weight too — about a pound a week. But in the exercising group, the dose of exercise required was nearly an hour a day of moderate-intensity activity, what the federal government currently recommends for weight loss but “a lot more than what many people would be able or willing to do,” Ravussin says.
At the same time, as many people have found after starting a new exercise regimen, working out can have a significant effect on appetite. The mechanisms that control appetite and energy balance in the human body are elegantly calibrated. “The body aims for homeostasis,” Braun says. It likes to remain at whatever weight it’s used to. So even small changes in energy balance can produce rapid changes in certain hormones associated with appetite, particularly acylated ghrelin, which is known to increase the desire for food, as well as insulin and leptin, hormones that affect how the body burns fuel.
The effects of exercise on the appetite and energy systems, however, are by no means consistent. In one study presented last year at the annual conference of the American College of Sports Medicine, when healthy young men ran for an hour and a half on a treadmill at a fairly high intensity, their blood concentrations of acylated ghrelin fell, and food held little appeal for the rest of that day. Exercise blunted their appetites. A study that Braun oversaw and that was published last year by The American Journal of Physiology had a slightly different outcome. In it, 18 overweight men and women walked on treadmills in multiple sessions while either eating enough that day to replace the calories burned during exercise or not. Afterward, the men displayed little or no changes in their energy-regulating hormones or their appetites, much as in the other study. But the women uniformly had increased blood concentrations of acylated ghrelin and decreased concentrations of insulin after the sessions in which they had eaten less than they had burned. Their bodies were directing them to replace the lost calories. In physiological terms, the results “are consistent with the paradigm that mechanisms to maintain body fat are more effective in women,” Braun and his colleagues wrote. In practical terms, the results are scientific proof that life is unfair. Female bodies, inspired almost certainly “by a biological need to maintain energy stores for reproduction,” Braun says, fight hard to hold on to every ounce of fat. Exercise for many women (and for some men) increases the desire to eat.
Thankfully there has lately been some more encouraging news about exercise and weight loss, including for women. In a study published late last month in The Journal of the American Medical Association, researchers from Harvard University looked at the weight-change histories of more than 34,000 participants in a women’s health study. The women began the study middle-aged (at an average of about 54 years) and were followed for 13 years. During that time, the women gained, on average, six pounds. Some packed on considerably more. But a small subset gained far less, coming close to maintaining the body size with which they started the study. Those were the women who reported exercising almost every day for an hour or so. The exercise involved was not strenuous. “It was the equivalent of brisk walking,” says I-Min Lee, a researcher at Harvard Medical School and diet until they lost an average of about 27 pounds each. Some of the women were then assigned to a walking program, some were put on a weight-training regimen and others were assigned no exercise; all returned to their old eating habits. Those who stuck with either of the exercise programs regained less weight than those who didn’t exercise and, even more striking, did not regain weight around their middles. The women who didn’t exercise regained their weight and preferentially packed on these new pounds around their abdomens. It’s well known that abdominal fat is particularly unhealthful, contributing significantly to metabolic disruptions and heart disease.
Scientists are “not really sure yet” just how and why exercise is so important in maintaining weight loss in people, Braun says. But in animal experiments, exercise seems to remodel the metabolic pathways that determine how the body stores and utilizes food. For a study published last summer, scientists at the University of Colorado at Denver fattened a group of male rats. The animals already had an inbred propensity to gain weight and, thanks to a high-fat diet laid out for them, they fulfilled that genetic destiny. After 16 weeks of eating as much as they wanted and lolling around in their cages, all were rotund. The scientists then switched them to a calorie-controlled, low-fat diet. The animals shed weight, dropping an average of about 14 percent of their corpulence.
Afterward the animals were put on a weight-maintenance diet. At the same time, half of them were required to run on a treadmill for about 30 minutes most days. The other half remained sedentary. For eight weeks, the rats were kept at their lower weights in order to establish a new base-line weight.
Then the fun began. For the final eight weeks of the experiment, the rats were allowed to relapse, to eat as much food as they wanted. The rats that had not been running on the treadmill fell upon the food eagerly. Most regained the weight they lost and then some.
But the exercising rats metabolized calories differently. They tended to burn fat immediately after their meals, while the sedentary rats’ bodies preferentially burned carbohydrates and sent the fat off to be stored in fat cells. The running rats’ bodies, meanwhile, also produced signals suggesting that they were satiated and didn’t need more kibble. Although the treadmill exercisers regained some weight, their relapses were not as extreme. Exercise “re-established the homeostatic steady state between intake and expenditure to defend a lower body weight,” the study authors concluded. Running had remade the rats’ bodies so that they ate less.
Streaming through much of the science and advice about exercise and weight loss is a certain Puritan streak, a sense that exercise, to be effective in keeping you slim, must be of almost medicinal dosage — an hour a day, every day; plenty of brisk walking; frequent long runs on the treadmill. But the very latest science about exercise and weight loss has a gentler tone and a more achievable goal. “Emerging evidence suggests that unlike bouts of moderate-vigorous activity, low-intensity ambulation, standing, etc., may contribute to daily energy expenditure without triggering the caloric compensation effect,” Braun wrote in the American College of Sports Medicine newsletter.
In a completed but unpublished study conducted in his energy-metabolism lab, Braun and his colleagues had a group of volunteers spend an entire day sitting. If they needed to visit the bathroom or any other location, they spun over in a wheelchair. Meanwhile, in a second session, the same volunteers stood all day, “not doing anything in particular,” Braun says, “just standing.” The difference in energy expenditure was remarkable, representing “hundreds of calories,” Braun says, but with no increase among the upright in their blood levels of ghrelin or other appetite hormones. Standing, for both men and women, burned multiple calories but did not ignite hunger. One thing is going to become clear in the coming years, Braun says: if you want to lose weight, you don’t necessarily have to go for a long run. “Just get rid of your chair.”
Weighing the Evidence on Exercise
By GRETCHEN REYNOLDS
How exercise affects body weight is one of the more intriguing and vexing issues in physiology. Exercise burns calories, no one doubts that, and so it should, in theory, produce weight loss, a fact that has prompted countless people to undertake exercise programs to shed pounds. Without significantly changing their diets, few succeed. “Anecdotally, all of us have been cornered by people claiming to have spent hours each week walking, running, stair-stepping, etc., and are displeased with the results on the scale or in the mirror,” wrote Barry Braun, an associate professor of kinesiology at the University of Massachusetts at Amherst, in the American College of Sports Medicine’s February newsletter.
But a growing body of science suggests that exercise does have an important role in weight loss. That role, however, is different from what many people expect and probably wish. The newest science suggests that exercise alone will not make you thin, but it may determine whether you stay thin, if you can achieve that state. Until recently, the bodily mechanisms involved were mysterious. But scientists are slowly teasing out exercise’s impact on metabolism, appetite and body composition, though the consequences of exercise can vary. Women’s bodies, for instance, seem to react differently than men’s bodies to the metabolic effects of exercise. None of which is a reason to abandon exercise as a weight-loss tool. You just have to understand what exercise can and cannot do.
“In general, exercise by itself is pretty useless for weight loss,” says Eric Ravussin, a professor at the Pennington Biomedical Research Center in Baton Rouge, La., and an expert on weight loss. It’s especially useless because people often end up consuming more calories when they exercise. The mathematics of weight loss is, in fact, quite simple, involving only subtraction. “Take in fewer calories than you burn, put yourself in negative energy balance, lose weight,” says Braun, who has been studying exercise and weight loss for years. The deficit in calories can result from cutting back your food intake or from increasing your energy output — the amount of exercise you complete — or both. When researchers affiliated with the Pennington center had volunteers reduce their energy balance for a study last year by either cutting their calorie intakes by 25 percent or increasing their daily exercise by 12.5 percent and cutting their calories by 12.5 percent, everyone involved lost weight. They all lost about the same amount of weight too — about a pound a week. But in the exercising group, the dose of exercise required was nearly an hour a day of moderate-intensity activity, what the federal government currently recommends for weight loss but “a lot more than what many people would be able or willing to do,” Ravussin says.
At the same time, as many people have found after starting a new exercise regimen, working out can have a significant effect on appetite. The mechanisms that control appetite and energy balance in the human body are elegantly calibrated. “The body aims for homeostasis,” Braun says. It likes to remain at whatever weight it’s used to. So even small changes in energy balance can produce rapid changes in certain hormones associated with appetite, particularly acylated ghrelin, which is known to increase the desire for food, as well as insulin and leptin, hormones that affect how the body burns fuel.
The effects of exercise on the appetite and energy systems, however, are by no means consistent. In one study presented last year at the annual conference of the American College of Sports Medicine, when healthy young men ran for an hour and a half on a treadmill at a fairly high intensity, their blood concentrations of acylated ghrelin fell, and food held little appeal for the rest of that day. Exercise blunted their appetites. A study that Braun oversaw and that was published last year by The American Journal of Physiology had a slightly different outcome. In it, 18 overweight men and women walked on treadmills in multiple sessions while either eating enough that day to replace the calories burned during exercise or not. Afterward, the men displayed little or no changes in their energy-regulating hormones or their appetites, much as in the other study. But the women uniformly had increased blood concentrations of acylated ghrelin and decreased concentrations of insulin after the sessions in which they had eaten less than they had burned. Their bodies were directing them to replace the lost calories. In physiological terms, the results “are consistent with the paradigm that mechanisms to maintain body fat are more effective in women,” Braun and his colleagues wrote. In practical terms, the results are scientific proof that life is unfair. Female bodies, inspired almost certainly “by a biological need to maintain energy stores for reproduction,” Braun says, fight hard to hold on to every ounce of fat. Exercise for many women (and for some men) increases the desire to eat.
Thankfully there has lately been some more encouraging news about exercise and weight loss, including for women. In a study published late last month in The Journal of the American Medical Association, researchers from Harvard University looked at the weight-change histories of more than 34,000 participants in a women’s health study. The women began the study middle-aged (at an average of about 54 years) and were followed for 13 years. During that time, the women gained, on average, six pounds. Some packed on considerably more. But a small subset gained far less, coming close to maintaining the body size with which they started the study. Those were the women who reported exercising almost every day for an hour or so. The exercise involved was not strenuous. “It was the equivalent of brisk walking,” says I-Min Lee, a researcher at Harvard Medical School and diet until they lost an average of about 27 pounds each. Some of the women were then assigned to a walking program, some were put on a weight-training regimen and others were assigned no exercise; all returned to their old eating habits. Those who stuck with either of the exercise programs regained less weight than those who didn’t exercise and, even more striking, did not regain weight around their middles. The women who didn’t exercise regained their weight and preferentially packed on these new pounds around their abdomens. It’s well known that abdominal fat is particularly unhealthful, contributing significantly to metabolic disruptions and heart disease.
Scientists are “not really sure yet” just how and why exercise is so important in maintaining weight loss in people, Braun says. But in animal experiments, exercise seems to remodel the metabolic pathways that determine how the body stores and utilizes food. For a study published last summer, scientists at the University of Colorado at Denver fattened a group of male rats. The animals already had an inbred propensity to gain weight and, thanks to a high-fat diet laid out for them, they fulfilled that genetic destiny. After 16 weeks of eating as much as they wanted and lolling around in their cages, all were rotund. The scientists then switched them to a calorie-controlled, low-fat diet. The animals shed weight, dropping an average of about 14 percent of their corpulence.
Afterward the animals were put on a weight-maintenance diet. At the same time, half of them were required to run on a treadmill for about 30 minutes most days. The other half remained sedentary. For eight weeks, the rats were kept at their lower weights in order to establish a new base-line weight.
Then the fun began. For the final eight weeks of the experiment, the rats were allowed to relapse, to eat as much food as they wanted. The rats that had not been running on the treadmill fell upon the food eagerly. Most regained the weight they lost and then some.
But the exercising rats metabolized calories differently. They tended to burn fat immediately after their meals, while the sedentary rats’ bodies preferentially burned carbohydrates and sent the fat off to be stored in fat cells. The running rats’ bodies, meanwhile, also produced signals suggesting that they were satiated and didn’t need more kibble. Although the treadmill exercisers regained some weight, their relapses were not as extreme. Exercise “re-established the homeostatic steady state between intake and expenditure to defend a lower body weight,” the study authors concluded. Running had remade the rats’ bodies so that they ate less.
Streaming through much of the science and advice about exercise and weight loss is a certain Puritan streak, a sense that exercise, to be effective in keeping you slim, must be of almost medicinal dosage — an hour a day, every day; plenty of brisk walking; frequent long runs on the treadmill. But the very latest science about exercise and weight loss has a gentler tone and a more achievable goal. “Emerging evidence suggests that unlike bouts of moderate-vigorous activity, low-intensity ambulation, standing, etc., may contribute to daily energy expenditure without triggering the caloric compensation effect,” Braun wrote in the American College of Sports Medicine newsletter.
In a completed but unpublished study conducted in his energy-metabolism lab, Braun and his colleagues had a group of volunteers spend an entire day sitting. If they needed to visit the bathroom or any other location, they spun over in a wheelchair. Meanwhile, in a second session, the same volunteers stood all day, “not doing anything in particular,” Braun says, “just standing.” The difference in energy expenditure was remarkable, representing “hundreds of calories,” Braun says, but with no increase among the upright in their blood levels of ghrelin or other appetite hormones. Standing, for both men and women, burned multiple calories but did not ignite hunger. One thing is going to become clear in the coming years, Braun says: if you want to lose weight, you don’t necessarily have to go for a long run. “Just get rid of your chair.”
What’s the Single Best Exercise?
By Gretchen Reynolds : NY Times : April 15, 2011
Let’s consider the butterfly. One of the most taxing movements in sports, the butterfly requires greater energy than bicycling at 14 miles per hour, running a 10-minute mile, playing competitive basketball or carrying furniture upstairs. It burns more calories, demands larger doses of oxygen and elicits more fatigue than those other activities, meaning that over time it should increase a swimmer’s endurance and contribute to weight control.
So is the butterfly the best single exercise that there is? Well, no. The butterfly “would probably get my vote for the worst” exercise, said Greg Whyte, a professor of sport and exercise science at Liverpool John Moores University in England and a past Olympian in the modern pentathlon, known for his swimming. The butterfly, he said, is “miserable, isolating, painful.” It requires a coach, a pool and ideally supplemental weight and flexibility training to reduce the high risk of injury.
Ask a dozen physiologists which exercise is best, and you’ll get a dozen wildly divergent replies. “Trying to choose” a single best exercise is “like trying to condense the entire field” of exercise science, said Martin Gibala, the chairman of the department of kinesiology at McMaster University in Hamilton, Ontario.
But when pressed, he suggested one of the foundations of old-fashioned calisthenics: the burpee, in which you drop to the ground, kick your feet out behind you, pull your feet back in and leap up as high as you can. “It builds muscles. It builds endurance.” He paused. “But it’s hard to imagine most people enjoying” an all-burpees program, “or sticking with it for long.”
And sticking with an exercise is key, even if you don’t spend a lot of time working out. The health benefits of activity follow a breathtakingly steep curve. “The majority of the mortality-related benefits” from exercising are due to the first 30 minutes of exercise, said Timothy Church, M.D., who holds the John S. McIlhenny endowed chair in health wisdom at the Pennington Biomedical Research Center in Baton Rouge, La. A recent meta-analysis of studies about exercise and mortality showed that, in general, a sedentary person’s risk of dying prematurely from any cause plummeted by nearly 20 percent if he or she began brisk walking (or the equivalent) for 30 minutes five times a week. If he or she tripled that amount, for instance, to 90 minutes of exercise four or five times a week, his or her risk of premature death dropped by only another 4 percent. So the one indisputable aspect of the single best exercise is that it be sustainable. From there, though, the debate grows heated.
“I personally think that brisk walking is far and away the single best exercise,” said Michael Joyner, M.D., a professor of anesthesiology at the Mayo Clinic in Rochester, Minn., and a leading researcher in the field of endurance exercise.
As proof, he points to the work of Hiroshi Nose, M.D., Ph.D., a professor of sports medical sciences at Shinshu University Graduate School of Medicine in Japan, who has enrolled thousands of older Japanese citizens in an innovative, five-month-long program of brisk, interval-style walking (three minutes of fast walking, followed by three minutes of slower walking, repeated 10 times). The results have been striking. “Physical fitness — maximal aerobic power and thigh muscle strength — increased by about 20 percent,” Dr. Nose wrote in an e-mail, “which is sure to make you feel about 10 years younger than before training.” The walkers’ “symptoms of lifestyle-related diseases (hypertension, hyperglycemia and obesity) decreased by about 20 percent,” he added, while their depression scores dropped by half.
Walking has also been shown by other researchers to aid materially in weight control. A 15-year study found that middle-aged women who walked for at least an hour a day maintained their weight over the decades. Those who didn’t gained weight. In addition, a recent seminal study found that when older people started a regular program of brisk walking, the volume of their hippocampus, a portion of the brain involved in memory, increased significantly.
But let’s face it, walking holds little appeal — or physiological benefit — for anyone who already exercises. “I nominate the squat,” said Stuart Phillips, Ph.D., a professor of kinesiology at McMaster University and an expert on the effects of resistance training on the human body. The squat “activates the body’s biggest muscles, those in the buttocks, back and legs.” It’s simple. “Just fold your arms across your chest,” he said, “bend your knees and lower your trunk until your thighs are about parallel with the floor. Do that 25 times. It’s a very potent exercise.” Use a barbell once the body-weight squats grow easy.
The squat, and weight training in general, are particularly good at combating sarcopenia, he said, or the inevitable and debilitating loss of muscle mass that accompanies advancing age. “Each of us is experiencing sarcopenia right this minute,” he said. “We just don’t realize it.” Endurance exercise, he added, unlike resistance training, does little to slow the condition.
Resistance training is good for weight control, as well. In studies conducted by other researchers, a regimen of simple weight training by sedentary men and women led to a significant decrease in waist circumference and abdominal fat. It also has been found to lower the risk of developing diabetes and cardiovascular disease. Counterintuitively, weight training may even improve cardiovascular fitness, Phillips said, as measured by changes in a person’s VO2max, or the maximum amount of oxygen that the heart and lungs can deliver to the muscles. Most physiologists believe that only endurance-exercise training can raise someone’s VO2max. But in small experiments, he said, weight training, by itself, effectively increased cardiovascular fitness.
“I used to run marathons,” he said. Now he mostly weight-trains, “and I’m in better shape.”
But there’s something undignified and boring about a squats-only routine. And the science supporting weight training as an all-purpose exercise approach, while provocative, remains inconclusive. Is there a single activity that has proved to be, at once, more strenuous than walking while building power like the squat?
“I think, actually, that you can make a strong case for H.I.T.,” Gibala said. High-intensity interval training, or H.I.T. as it’s familiarly known among physiologists, is essentially all-interval exercise. As studied in Gibala’s lab, it involves grunting through a series of short, strenuous intervals on specialized stationary bicycles, known as Wingate ergometers. In his first experiments, riders completed 30 seconds of cycling at the highest intensity the riders could stand. After resting for four minutes, the volunteers repeated the interval several times, for a total of two to three minutes of extremely intense exercise. After two weeks, the H.I.T. riders, with less than 20 minutes of hard effort behind them, had increased their aerobic capacity as much as riders who had pedaled leisurely for more than 10 hours. Other researchers also have found that H.I.T. reduces blood-sugar levels and diabetes risk, and Gibala anticipates that it will aid in weight control, although he hasn’t studied that topic fully yet.
The approach seems promising, since most of us have minimal time to exercise each week. Gibala last month published a new study of H.I.T., requiring only a stationary bicycle and some degree of grit. In this modified version, you sprint for 60 seconds at a pace that feels unpleasant but sustainable, followed by 60 seconds of pedaling easily, then another 60-second sprint and recovery, 10 times in all. “There’s no particular reason why” H.I.T. shouldn’t be adaptable to almost any sport, Gibala said, as long as you adequately push yourself.
Of course, to be effective, H.I.T. must hurt. But a study published last month found that when a group of recreational runners practiced H.I.T. on the track, they enjoyed the workout more than a second group of runners who jogged continuously for 50 minutes. The H.I.T. runners, the study’s authors suspect, were less bored.
The only glaring inadequacy of H.I.T. is that it builds muscular strength less effectively than, say, the squat. But even that can be partially remedied, Gibala said: “Sprinting up stairs is a power workout and interval session simultaneously.”Meaning that running up steps just might be the single best exercise of all. Great news for those of us who could never master the butterfly.