VITAMIN B 12 DEFICIENCY
Causes of Vitamin B12 Deficiency
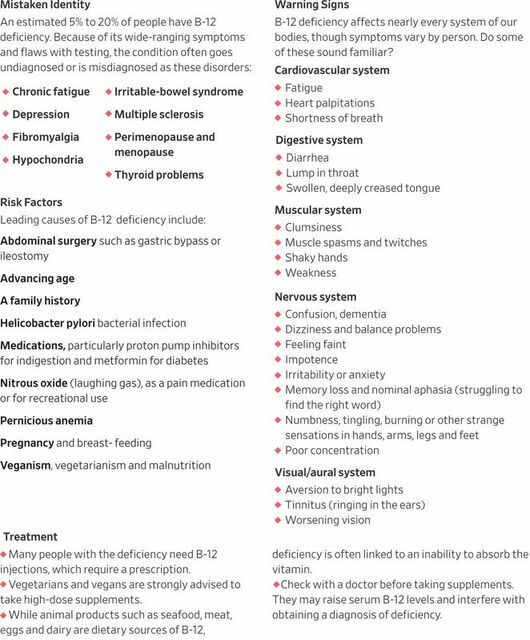
Vitamin B12 deficiency can have a number of possible causes. Typically it occurs in people whose digestive systems do not adequately absorb the vitamin from the foods they eat. This can be caused by:
Babies born to mothers who are vegetarians may also be deficient in vitamin B12.
Vitamin B12 deficiency can have a number of possible causes. Typically it occurs in people whose digestive systems do not adequately absorb the vitamin from the foods they eat. This can be caused by:
- Pernicious anemia, a condition in which there is a lack of a protein called intrinsic factor. The protein, which is made in the stomach, is necessary for vitamin B12 absorption.
- Atrophic gastritis, a thinning of the stomach lining that affects up to 30% of people aged 50 and older.
- Surgery in which part of the stomach and/or small intestine is removed.
- Conditions affecting the small intestine, such as Crohn's disease, celiac disease, bacterial growth, or a parasite.
- Excessive alcohol consumption.
- Autoimmune disorders, such as Graves' disease or systemic lupus erythematosus
- Long-term use of certain drugs eg acid-reducing drugs (Prilosec/Nexium) and metformin used by many diabetics
Babies born to mothers who are vegetarians may also be deficient in vitamin B12.
It Could Be Old Age, or It Could Be Low B12
By Jane E. Brody : NY Times : November 28, 2011
Ilsa Katz was 85 when her daughter, Vivian Atkins, first noticed that her mother was becoming increasingly confused.
“She couldn’t remember names, where she’d been or what she’d done that day,” Ms. Atkins recalled in an interview. “Initially, I was not too worried. I thought it was part of normal aging. But over time, the confusion and memory problems became more severe and more frequent.”
Her mother couldn’t remember the names of close relatives or what day it was. She thought she was going to work or needed to go downtown, which she never did. And she was often agitated.
A workup at a memory clinic resulted in a diagnosis of early Alzheimer’s disease, and Ms. Katz was prescribed Aricept, which Ms. Atkins said seemed to make matters worse. But the clinic also tested Ms. Katz’s blood level of vitamin B12. It was well below normal, and her doctor thought that could be contributing to her symptoms.
Weekly B12 injections were begun. “Soon afterward, she became less agitated, less confused and her memory was much better,” said Ms. Atkins. “I felt I had my mother back, and she feels a lot better, too.”
Now 87, Ms. Katz still lives alone in Manhattan and feels well enough to refuse outside assistance.
Still, her daughter wondered, “Why aren’t B12 levels checked routinely, particularly in older people?”
It is an important question. As we age, our ability to absorb B12 from food declines, and often so does our consumption of foods rich in this vitamin. A B12 deficiency can creep up without warning and cause a host of confusing symptoms that are likely to be misdiagnosed or ascribed to aging.
A Vital Nutrient
B12 is an essential vitamin with roles throughout the body. It is needed for the development and maintenance of a healthy nervous system, the production of DNA and formation of red blood cells.
A severe B12 deficiency results in anemia, which can be picked up by an ordinary blood test. But the less dramatic symptoms of a B12 deficiency may include muscle weakness, fatigue, shakiness, unsteady gait, incontinence, low blood pressure, depression and other mood disorders, and cognitive problems like poor memory.
Labs differ in what they consider normal, but most authorities say a deficiency occurs when B12 levels in adults fall below 250 picograms per milliliter of blood serum. Like all B vitamins, B12 is water-soluble, but the body stores extra B12 in the liver and other tissues. Even if dietary sources are inadequate for some time, a serum deficiency may not show up for years.
If the amount of B12 in storage is low to begin with, a deficiency can develop within a year, even more quickly in infants.
Recommended dietary amounts of B12 vary: 2.4 micrograms daily for those age 14 and older, 2.6 micrograms for pregnant women and 2.8 micrograms for nursing women. Barring circumstances that impair B12 absorption, these are levels easily obtained from a well-balanced dietcontaining animal protein.
In its natural form, B12 is present in significant amounts only in animal foods, most prominently in liver (83 micrograms in a 3.5-ounce serving). Good food sources include other red meats, turkey, fish and shellfish. Lesser amounts of the vitamin are present in dairy products, eggs and chicken.
Those at Risk
Natural plant sources are meager at best in B12, and the vitamin is poorly absorbed from them. Many strict vegetarians and all vegans, as well as infants they breast-feed, must consume supplements or fortified breakfast cereals to get adequate amounts.
Certain organisms, like the bacterium Spirulina and some algae, contain a pseudo-B12 that the body cannot use but may result in a false reading of a normal B12 level on a blood test. Despite claims to the contrary, laver, a seaweed, and barley grass are not reliable sources of B12.
In animal foods, B12 is combined with protein and must be released by stomach acid and an enzyme to be absorbed. Thus, chronic users of acid-suppressing drugs like Prilosec, Prevacid and Nexium, as well as ulcer medications like Pepcid and Tagamet, are at risk of developing a B12 deficiency and often require a daily B12 supplement.
Stomach acid levels decline with age. As many as 30 percent of older people may lack sufficient stomach acid to absorb adequate amounts of B12 from natural sources. Therefore, regular consumption of fortified foods or supplementation with 25 to 100 micrograms of B12 daily is recommended for people over 50.
Synthetic B12, found in supplements and fortified foods, does not depend on stomach acid to be absorbed. But whether natural or synthetic, only some of the B12 consumed gets into the body. Treatment to correct a B12 deficiency typically involves much larger doses than the body actually requires.
Free B12 from both natural and synthetic sources must be combined with a substance in the stomach called intrinsic factor to be absorbed through the gut. This factor is lacking in people with an autoimmune disorder called pernicious anemia; the resulting vitamin deficiency is commonly treated with injections of B12.
Although most doctors are quick to recommend injections to correct a B12 deficiency, considerable evidence indicates that, in large enough doses, sublingual (under-the-tongue) tablets or skin patches of B12 may work as well as injections for people with absorption problems, even for those with pernicious anemia.
Most often, a daily supplement of 2,000 micrograms is recommended for about a month, then lowered to 1,000 micrograms daily for another month, then lowered again to 1,000 micrograms weekly. Sublingual B12 or B12 patches, or even B12 lollipops, can be helpful for people who require a supplement but cannot swallow pills.
Others at risk of developing a B12 deficiency include heavy drinkers (alcohol diminishes B12 absorption), those who have had stomach surgery for weight loss or ulcers, and people who take aminosalicylic acid (for inflammatory bowel disease or tuberculosis) or the diabetes drug metformin (sold as Glucophage and other brands). Patients who take the anticonvulsants phenytoin, phenobarbital or primidone are also at risk.
Large doses of folic acid can mask a B12 deficiency and cause permanent neurological damage if normal levels of B12 are not maintained. Supplements of potassium impair B12 absorption in some people.
Although a B12 deficiency can raise blood levels of the amino acid homocysteine, a risk factor for heart disease and stroke, supplements of B12 have not reduced cardiovascular risk.
And while high homocysteine levels are linked to Alzheimer’s disease and dementia, lowering them with B12 supplements has not been shown to improve cognitive function. However, in one study, among women with a poor dietary intake of B12, supplements of the vitamin significantly slowed the rate of cognitive decline.
By Jane E. Brody : NY Times : November 28, 2011
Ilsa Katz was 85 when her daughter, Vivian Atkins, first noticed that her mother was becoming increasingly confused.
“She couldn’t remember names, where she’d been or what she’d done that day,” Ms. Atkins recalled in an interview. “Initially, I was not too worried. I thought it was part of normal aging. But over time, the confusion and memory problems became more severe and more frequent.”
Her mother couldn’t remember the names of close relatives or what day it was. She thought she was going to work or needed to go downtown, which she never did. And she was often agitated.
A workup at a memory clinic resulted in a diagnosis of early Alzheimer’s disease, and Ms. Katz was prescribed Aricept, which Ms. Atkins said seemed to make matters worse. But the clinic also tested Ms. Katz’s blood level of vitamin B12. It was well below normal, and her doctor thought that could be contributing to her symptoms.
Weekly B12 injections were begun. “Soon afterward, she became less agitated, less confused and her memory was much better,” said Ms. Atkins. “I felt I had my mother back, and she feels a lot better, too.”
Now 87, Ms. Katz still lives alone in Manhattan and feels well enough to refuse outside assistance.
Still, her daughter wondered, “Why aren’t B12 levels checked routinely, particularly in older people?”
It is an important question. As we age, our ability to absorb B12 from food declines, and often so does our consumption of foods rich in this vitamin. A B12 deficiency can creep up without warning and cause a host of confusing symptoms that are likely to be misdiagnosed or ascribed to aging.
A Vital Nutrient
B12 is an essential vitamin with roles throughout the body. It is needed for the development and maintenance of a healthy nervous system, the production of DNA and formation of red blood cells.
A severe B12 deficiency results in anemia, which can be picked up by an ordinary blood test. But the less dramatic symptoms of a B12 deficiency may include muscle weakness, fatigue, shakiness, unsteady gait, incontinence, low blood pressure, depression and other mood disorders, and cognitive problems like poor memory.
Labs differ in what they consider normal, but most authorities say a deficiency occurs when B12 levels in adults fall below 250 picograms per milliliter of blood serum. Like all B vitamins, B12 is water-soluble, but the body stores extra B12 in the liver and other tissues. Even if dietary sources are inadequate for some time, a serum deficiency may not show up for years.
If the amount of B12 in storage is low to begin with, a deficiency can develop within a year, even more quickly in infants.
Recommended dietary amounts of B12 vary: 2.4 micrograms daily for those age 14 and older, 2.6 micrograms for pregnant women and 2.8 micrograms for nursing women. Barring circumstances that impair B12 absorption, these are levels easily obtained from a well-balanced dietcontaining animal protein.
In its natural form, B12 is present in significant amounts only in animal foods, most prominently in liver (83 micrograms in a 3.5-ounce serving). Good food sources include other red meats, turkey, fish and shellfish. Lesser amounts of the vitamin are present in dairy products, eggs and chicken.
Those at Risk
Natural plant sources are meager at best in B12, and the vitamin is poorly absorbed from them. Many strict vegetarians and all vegans, as well as infants they breast-feed, must consume supplements or fortified breakfast cereals to get adequate amounts.
Certain organisms, like the bacterium Spirulina and some algae, contain a pseudo-B12 that the body cannot use but may result in a false reading of a normal B12 level on a blood test. Despite claims to the contrary, laver, a seaweed, and barley grass are not reliable sources of B12.
In animal foods, B12 is combined with protein and must be released by stomach acid and an enzyme to be absorbed. Thus, chronic users of acid-suppressing drugs like Prilosec, Prevacid and Nexium, as well as ulcer medications like Pepcid and Tagamet, are at risk of developing a B12 deficiency and often require a daily B12 supplement.
Stomach acid levels decline with age. As many as 30 percent of older people may lack sufficient stomach acid to absorb adequate amounts of B12 from natural sources. Therefore, regular consumption of fortified foods or supplementation with 25 to 100 micrograms of B12 daily is recommended for people over 50.
Synthetic B12, found in supplements and fortified foods, does not depend on stomach acid to be absorbed. But whether natural or synthetic, only some of the B12 consumed gets into the body. Treatment to correct a B12 deficiency typically involves much larger doses than the body actually requires.
Free B12 from both natural and synthetic sources must be combined with a substance in the stomach called intrinsic factor to be absorbed through the gut. This factor is lacking in people with an autoimmune disorder called pernicious anemia; the resulting vitamin deficiency is commonly treated with injections of B12.
Although most doctors are quick to recommend injections to correct a B12 deficiency, considerable evidence indicates that, in large enough doses, sublingual (under-the-tongue) tablets or skin patches of B12 may work as well as injections for people with absorption problems, even for those with pernicious anemia.
Most often, a daily supplement of 2,000 micrograms is recommended for about a month, then lowered to 1,000 micrograms daily for another month, then lowered again to 1,000 micrograms weekly. Sublingual B12 or B12 patches, or even B12 lollipops, can be helpful for people who require a supplement but cannot swallow pills.
Others at risk of developing a B12 deficiency include heavy drinkers (alcohol diminishes B12 absorption), those who have had stomach surgery for weight loss or ulcers, and people who take aminosalicylic acid (for inflammatory bowel disease or tuberculosis) or the diabetes drug metformin (sold as Glucophage and other brands). Patients who take the anticonvulsants phenytoin, phenobarbital or primidone are also at risk.
Large doses of folic acid can mask a B12 deficiency and cause permanent neurological damage if normal levels of B12 are not maintained. Supplements of potassium impair B12 absorption in some people.
Although a B12 deficiency can raise blood levels of the amino acid homocysteine, a risk factor for heart disease and stroke, supplements of B12 have not reduced cardiovascular risk.
And while high homocysteine levels are linked to Alzheimer’s disease and dementia, lowering them with B12 supplements has not been shown to improve cognitive function. However, in one study, among women with a poor dietary intake of B12, supplements of the vitamin significantly slowed the rate of cognitive decline.
